
〒213-0002 神奈川県川崎市高津区二子1丁目7−17
リバーサイドマンション杉崎 102 二子新地駅 徒歩3分
| 月 | 火 | 水 | 木 | 金 | 土 | 日祝 | |
|---|---|---|---|---|---|---|---|
| 9:00〜13:00 | ● | ● | ● | ● | ● | ● | ─ |
| 15:00〜19:00 | ● | ● | ● | ● | ● | ● | ─ |
腰を反ると痛い原因と対処法
公開日:2026/03/13
更新日:2026/00/00
腰を反らす動作で痛みが生じる伸展型腰痛(EB-LBP)について、その発生機序から治療法までを包括的に解説しています。主な原因として、腰椎椎間関節症や脊椎分離症、脊柱管狭窄症などが挙げられ、これらは後方支持組織への過度な負荷によって引き起こされます。
治療面では、体幹の安定化運動や可動域の改善といった保存療法が推奨されており、特に若年アスリートへの有効性が強調されています。
また、厳格な安静を求める欧米の伝統的指針に対し、活動を継続しながら回復を目指す日本独自の進歩的なリハビリテーション手法についても言及されています。
全体を通して、正確な診断に基づき、個々の病態に合わせた段階的な運動療法を行うことの重要性が示されています。
目次
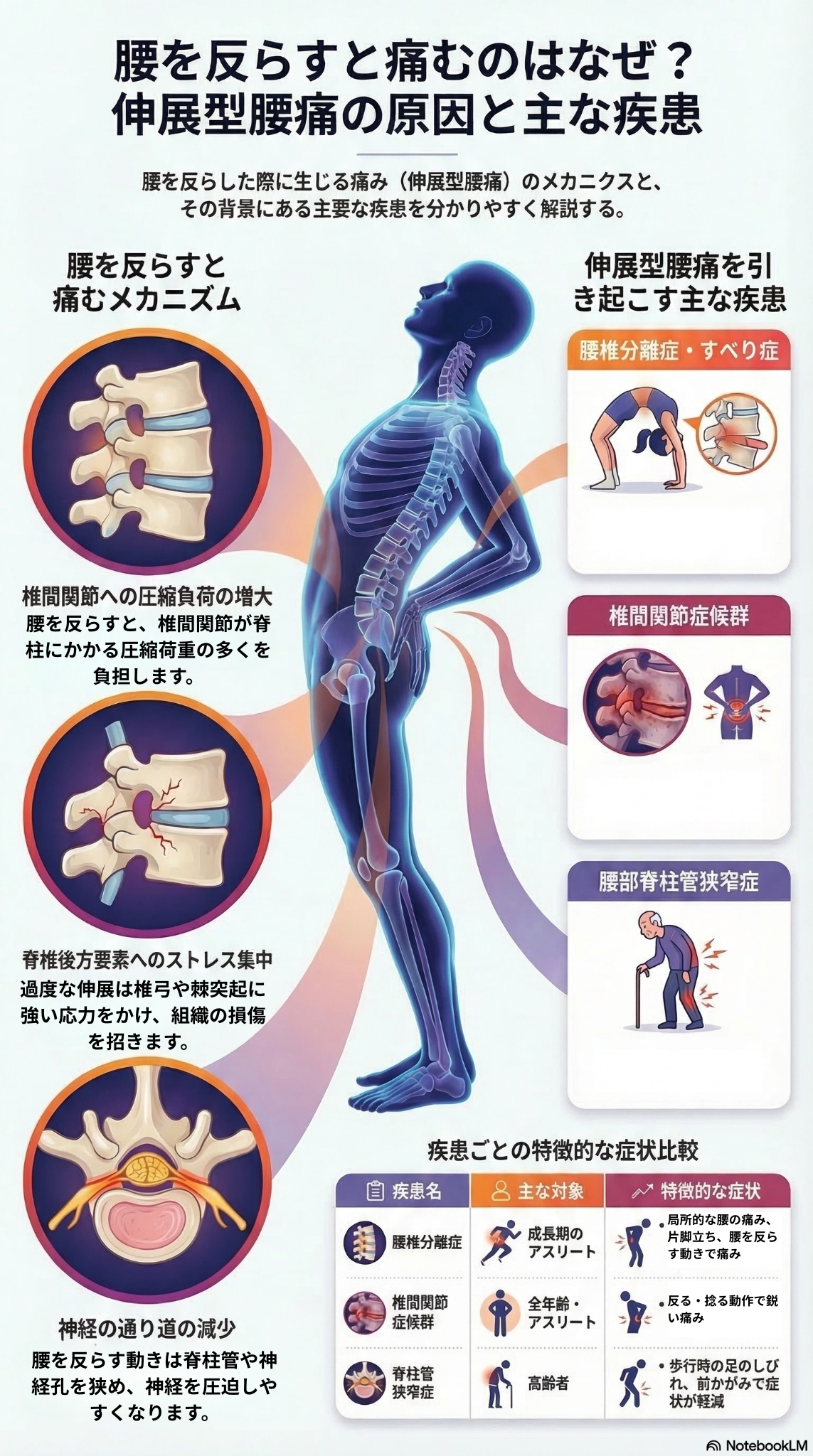
腰を反らす動作(伸展)によって引き起こされる、あるいは悪化する腰痛は「伸展型腰痛(Extension-based lower back pain: EB-LBP)」と呼ばれ、特定の病理学的要因を持つ疾患グループとして認識されています。
腰を反らす動作は、脊椎の後方要素への圧縮力や機械的負荷を著しく増加させるため、これらの組織にストレスがかかることが痛みの主な原因となります。
腰を反らすと痛む主な疾患と、そのメカニズムは以下の通りです。
- 原因・メカニズム: 背骨の後方にある「椎間関節」は、腰を過度に反らす(過伸展)際に脊椎にかかる圧縮荷重の大部分を支えるため、非常に強い負荷がかかります。加齢などによってこの関節に変形性関節症などの退行性変化が生じると、関節が硬くなり、滑膜の炎症や骨の浮腫を引き起こし、腰を反らした際の痛みの原因となります。
- 特徴: 慢性腰痛の15〜45%を占めると推定される一般的な原因です。体をひねったり、横に曲げたり、反らしたりすることで悪化する、深部がうずくような痛みが特徴です。
- 原因・メカニズム: 椎弓狭部(pars interarticularis)と呼ばれる骨の脆弱な部分に、伸展(反り)と回旋(ひねり)が組み合わさった反復的なストレスがかかることで生じる疲労骨折が主な原因です。
- 特徴: 思春期や若年層のアスリートにおける伸展型腰痛の最も一般的な原因です。野球の投球、体操、飛び込み、アメリカンフットボールなど、腰を反らす動作を繰り返すスポーツで特に多く見られます。腰を反らすなど特定の活動によって悪化し、休むと和らぐ局所的な痛みが特徴です。
- 原因・メカニズム: 加齢などに伴う退行性疾患であり、腰を反らす動作によって「黄色靭帯が内側にたわむ」「椎間関節が接近する」といった現象が起こります。これにより、神経の通り道である脊柱管や椎間孔のスペースがさらに狭まり、神経が圧迫されることで症状が悪化します。逆に前屈みになると、神経の通るスペースが広がります。
- 特徴: 歩行や起立時(腰が反る姿勢)に脚の痛み、しびれ、筋力低下が生じ、**座ったり前屈みになったりすると症状が改善する「間欠性跛行(神経性跛行)」**が典型的な症状です。
- 棘突起インピンジメント(Spinous Process Impaction): 極端に腰を反らした際に、隣り合う背骨の突起(棘突起)同士がぶつかり合い、局所的な痛みや骨髄浮腫、ストレス損傷を引き起こす比較的稀な疾患です。思春期のアスリートなどで報告されています。
これらの疾患を見分けるためには、問診(下り坂の歩行や頭上の物を取る動作など、腰を反らす活動で痛むか)のほか、片足立ちで腰を反らして痛みを誘発する「ストークテスト」などの身体診察、CTやMRIによる画像診断が重要です。
いずれの疾患においても、体幹(コアマッスルや多裂筋など)の安定性を高める運動療法、理学療法、活動の調整などの**「保存的治療」が第一選択として推奨されており、多くの患者において良好な結果が報告されています**。
「ストークテスト(Stork Test)」、別名「片足立ち腰椎伸展テスト(single-leg hyperextension test)」は、脊椎分離症などの診断において非常に重要な身体診察のテストです。
具体的なテストのやり方と、早期発見に役立つ理由は以下の通りです。
- 方法: 患者が**片足で立った状態で、腰を後ろに反らす(伸展させる)**動作を行います。
- 判定: この動作を行った際に、腰の特定の場所(局所)に痛みが誘発された場合、テストは「陽性」と判断されます。
ストークテストは、**脊椎分離症に対して高い感度(異常を正しく検出する能力)**を持っていることがわかっています。
若年層の分離症は「腰を反らす」動作によって背骨の後方の弱い部分(椎弓狭部)にストレスがかかることで生じます。ストークテストは、片足立ちになることで左右どちらかの背骨の関節にさらに負荷を集中させながら腰を反らすため、初期の疲労骨折やストレス反応による痛みを的確に引き出す(再現する)ことができます。
このテストで痛みが確認された場合、早期にCTやMRIなどの画像診断へ進むきっかけとなり、骨が完全に癒合する(くっつく)可能性が高い初期段階での治療開始につながります。
これまで、特に欧米などでは、3〜6ヶ月間のスポーツの完全な中止(休養)と、硬性コルセット(TLSOなど)による固定が標準的な治療とされてきました。痛みを誘発する活動を厳格に避けることが、保存的治療(手術をしない治療)の第一歩とされています。
一方で、日本の最新の臨床研究では、**「スポーツ活動を厳格に制限しない段階的なリハビリテーション」**の有効性が示されています。
- 完全に休養してしまうと、筋力低下(デコンディショニング)や筋萎縮、アスリートにとっての心理的なストレスやアイデンティティの喪失を引き起こす悪影響があると考えられているためです。
- この日本のアプローチでは、症状を慎重にモニタリングしながら、技術や練習量を調整し、完全な休養ではなくスポーツへの参加を継続します。
完全休養を避ける場合でも、無制限にスポーツをして良いわけではありません。以下の点に注意する必要があります。
- 痛みを伴う動作(特に腰を反らす動作)の回避: 急性期や回復期においては、痛みを誘発する「腰を反らす(伸展)動作」を避けるように活動を調整することが非常に重要です。
- 体幹の安定性と柔軟性の向上: リハビリでは、深部の腹筋や多裂筋などのコアマッスルを強化し、股関節の屈筋やハムストリングス(太もも裏)の柔軟性を改善することで、腰が過剰に反るのを防ぐ必要があります。
- 段階的な復帰: 痛みのない範囲で全身のコンディショニングを維持し、症状の改善に合わせて一般的な運動からスポーツ特有の動作へと段階的に負荷を増やしていきます。
多くの若いアスリートは、正確な診断と適切な保存的治療により、スポーツに完全復帰できることがわかっています。完全に休むべきか、練習メニューを調整しながらリハビリを行うかは、症状の重症度や医師の判断によるため、まずは担当医や理学療法士と相談し、**「痛みを伴わない範囲での活動の調整」**を個別に行うことが推奨されます。
脊椎分離症の治療において、骨の癒合(くっつくこと)を期待してコルセット(TLSOなどの硬性装具)を使用する場合、一般的なプロトコルでは3〜6ヶ月間の装着が推奨されています。
- 装着時間と過程: 基本的には1日23時間のフルタイム装着を行い、背骨の動きを制限して痛みを和らげながら治癒を促します。その後、症状の改善や画像診断での回復具合を確認しながら、徐々に装着時間を減らしていくのが一般的です。
- 近年の治療動向: ただし、コルセットの役割については現在議論があります。3〜6ヶ月間もの長期間固定し続けると、筋力低下や運動制御能力への悪影響(デコンディショニング)が生じる可能性があるためです。
現在では患者の年齢、活動レベル、症状の重さに応じて、コルセットを使用せずに痛みの出る動作(特に腰を反らす動作)を厳格に避けながら、理学療法(リハビリ)を中心に行うアプローチでも同等の回復が得られるケースがあることが示されています。
腰が反る(過伸展)のを防ぐための体幹トレーニングは、主に**「深部の腹筋群」と「多裂筋(背骨を直接支える筋肉)」の強化**をターゲットとして行われます。
文献で推奨されている具体的なトレーニングのアプローチや考え方は以下の通りです。
ハムストリングス(太ももの裏側)や股関節の屈筋群(脚の付け根)が硬いと、日常の動作やスポーツ中に**「代償的な腰の過伸展(無理に腰を反らせる動作)」を引き起こしてしまう**ため、腰に悪影響を及ぼします。
具体的なメカニズムは以下の通りです。
- 腰への過剰な負荷の集中: ハムストリングスや股関節周りの筋肉が硬いと、股関節周辺の柔軟性が制限されます。その結果、脚や骨盤を動かすべき場面で十分な動きができず、身体が無意識のうちに腰の骨(腰椎)を過剰に反らせることで足りない動きを補おうとしてしまいます(代償動作)。
- 背骨の組織への物理的ストレス: このように腰が過剰に反る(過伸展)状態が続くと、背骨の後方要素(椎間関節や椎弓など)に過度な機械的負荷が集中してかかり、分離症や椎間関節症などの痛みの原因となります。
実際に、小児の腰椎分離症患者を対象とした研究では、70%の患者にハムストリングスの硬さ、85%に股関節屈筋の硬さが見られたことが報告されています。
若年アスリート(特に野球、体操、飛び込み、アメリカンフットボールなど腰を反らす動作が多い競技)における伸展型腰痛(脊椎分離症など)の運動療法と予防策は、単に休むだけでなく、痛みの原因となる生体力学的な負荷を取り除くことに重点が置かれます。
文献で推奨されている若年アスリート向けの具体的な運動療法と予防策は以下の通りです。
- モーターコントロール(運動制御)と体幹の安定化: 単に腹筋や背筋の筋力を強化するだけでなく、骨盤をニュートラルな位置に保ちながら、深部の腹筋群と腰部の多裂筋(背骨を支える筋肉)を正しく機能させる訓練が不可欠です**,,。痛みの神経回路を落ち着かせるためのコントロール能力の改善が重視されます**。
- 股関節周りの徹底的な柔軟性改善: 若年アスリートの腰痛では、股関節の屈筋群(腸腰筋など)や太もも裏(ハムストリングス)の硬さが、代償的な腰の過伸展(反りすぎ)を引き起こす主要な原因となります**,。そのため、これらの筋肉のストレッチは運動療法の中心的な要素となります,**。
- 屈曲ベース(腰を丸める)エクササイズ: 急性期には痛みを誘発する「腰を反らす動作」を厳格に避け、背骨の負担を減らしながら機能を維持するために、腰を曲げる・丸める方向への理学療法が第一選択となります**,**。
- 段階的なスポーツ復帰(プログレッシブ・リハビリテーション): 痛みのない範囲で全身のコンディショニングを維持し、一般的な運動からスポーツ特有の動作へと段階的に負荷を増やしていきます**,。特に日本の臨床現場では、完全な休養による筋力低下(デコンディショニング)や心理的悪影響を防ぐため、が有効とされています,,**。
- 技術(フォーム)の修正: スポーツ特有の動作において、腰に過度な負担がかかるフォームを修正します**。例えば、野球の投球動作では、極端な腰の伸展(反り)と回旋(ひねり)の組み合わせが分離症の大きなリスクとなるため、生体力学的な負担を減らす動作改善が必要です,,**。
- 身体的機能不全の早期評価と改善: 痛みが出る前に、股関節屈筋やハムストリングスの硬さ、腹筋や多裂筋の弱さといった「身体的機能不全」を評価し、これらを柔軟性・筋力トレーニングで事前に修正しておくことがケガのリスク軽減につながります****。
- トレーニング負荷の管理: 成長期で骨が未熟な時期(特に椎弓狭部などの脆弱な部分)には、反復的なストレスによる疲労骨折が起きやすいため、練習の強度やボリュームを適切に管理することが重要です**,,**。
- 早期発見と介入: アスリート本人やコーチ、トレーナーが「腰を反らした時の痛み」を早期に認識することが極めて重要です**,,**。症状の発生から1ヶ月以内に早期診断されれば、保存的治療によって骨が完全に癒合する(くっつく)確率が非常に高くなります,。
野球の投球動作は、腰に対して「過度な伸展(反り)」と「回旋(ひねり)」という大きな負荷を生み出すため、脊椎分離症や椎間関節の炎症を引き起こすリスクが非常に高い動作の一つです。
文献で示されている生体力学的なメカニズムや予防戦略に基づくと、腰への負担を減らすフォームや身体の使い方のコツとして以下の点が挙げられます。
投球動作は、強い伸展(腰を反らす)と回旋(腰をひねる)の力、そして高いねじりトルクを生み出し、これが背骨の後方の弱い部分(椎弓狭部)や椎間関節に直接的なストレスを集中させます。
投球フォームの修正においては、腰椎(腰の骨)だけで無理に身体を大きく反らしたりひねったりする極端な動作(ハイパーエクステンション)を避け、生体力学的な負荷を減らす技術修正が必要です。
前回の会話でも触れた通り、股関節の屈筋群(脚の付け根)やハムストリングス(太もも裏)が硬いと、脚を動かす際に股関節が十分に機能せず、その足りない動きを補うために**「無意識のうちに腰を過剰に反らせてしまう(代償的な腰椎の過伸展)」**という現象が起きます。
体重移動(並進運動)や踏み込みの際に腰へ負担をかけないよう、股関節周りの柔軟性を徹底的に高め、腰ではなく「股関節の可動域をしっかり生かしたフォーム」を作ることが不可欠です。
投球時の強い負荷から腰を守るためには、深部の腹筋群と多裂筋(背骨を支える筋肉)を機能させ、骨盤をニュートラル(過度な反り腰にならない中間位置)に保つ能力が求められます。
体幹が不安定なまま腕を振ると腰が過剰に反りやすくなるため、体幹の筋肉をコルセットのように安定させた状態で投球動作を行うことが負担軽減につながります。
投球フォームにおける腰への負担を減らすには、単に投げ方の見た目をいじるだけでなく、「股関節の硬さ」や「体幹の不安定さ」といった身体的な機能不全を事前に修正することが根本的な解決策となります。
腰が無理に反らなくても全身の連動で力強いボールが投げられる状態を作ることが、分離症などの怪我を予防する最大のコツです。
日本と欧米のリハビリ(保存的治療)手法における最も大きな違いは、**「スポーツ活動の制限(休養)に対する考え方」**にあります。
- 長期のスポーツ完全中止: 伝統的な欧米のプロトコルでは、3〜6ヶ月間という長期間にわたってスポーツ活動を完全に中止(完全休養)することが強調されてきました。
- 装具による固定: 急性期の分離症などに対しては、硬性コルセット(TLSOなど)を1日23時間装着し、背骨の動きを制限して治癒を促す手法が一般的に用いられます。
- 完全な制限を避ける段階的リハビリ: 日本の臨床現場では、スポーツ活動を厳格に制限する(完全に休む)ことなく、段階的にリハビリテーションを進めるアプローチが特徴的です。
- 活動の調整と継続: スポーツを完全にやめるのではなく、症状を慎重にモニタリングしながら、痛みを誘発する動作を避け、練習量やフォーム(技術)を調整しつつ競技への参加を継続します。
- 運動療法への強い重点: 日本の文献では、自宅での毎日のセルフストレッチ(特に股関節屈筋やハムストリングス)と、通院での体幹トレーニングやエアロバイクなどを組み合わせた、積極的な理学療法・運動療法が強く推奨されています。
日本のアプローチは、長期間の完全な休息がもたらす筋力低下や身体機能の低下(デコンディショニング)、筋萎縮、そして「スポーツができない」ことによるアスリートの心理的苦痛を避けることを目的としています。
[1] Yu, C. C., et al. (2011). Spondylolysis and Spondylolisthesis in Baseball Athletes: Five case reports. DOI: 10.6315/2011.39(1)06
[2] Matsuzawa, Y., et al. Effectiveness of a Progressive Rehabilitation Approach Without Sport Activity Restriction for Acute Lumbar Spondylolysis in High-Level Athletes: A Retrospective Case Series.
[3] Winslow, J., et al. (2018). Rehabilitation of a Young Athlete With Extension-Based Low Back Pain Addressing Motor-Control Impairments and Central Sensitization. Journal of Athletic Training. DOI: 10.4085/1062-6050-238-16
[4] Mohile, N., et al. (2022). Spondylolysis and Isthmic Spondylolisthesis: A Guide to Diagnosis and Management. Journal of the American Board of Family Medicine. DOI: 10.3122/jabfm.2022.220130R1
[5] Kim, H. J., et al. (2018). Factors Associated with the Symptoms of Young Adults with L5 Spondylolysis. Asian Spine Journal. DOI: 10.4184/ASJ.2018.12.3.476
[6] Cohen, S. P., et al. (2007). Pathogenesis, Diagnosis, and Treatment of Lumbar Zygapophysial (Facet) Joint Pain. Anesthesiology. DOI: 10.1097/00000542-200703000-00024
[7] Fukuda, T., et al. (2025). Lumbar Spinous Process Impaction Injuries Caused by Extension Stress in Adolescent Athletes: A Report of Two Cases. Cureus. DOI: 10.7759/cureus.84363
[8] Brearley, S., et al. (2021). Inter-Disciplinary Conservative Management of Bilateral Non-United Lumbar Pars Defects in a Junior Elite Golfer. The International Journal of Sports Physical Therapy. DOI: 10.26603/001C.18873
[9] Cavanaugh, J. M., et al. (1996). Lumbar facet pain: biomechanics, neuroanatomy and neurophysiology. Journal of Biomechanics. DOI: 10.1016/0021-9290(96)00023-1
[10] King, A. I., et al. (1984). Mechanism of facet load transmission as a hypothesis for low-back pain. Spine. DOI: 10.1097/00007632-198409000-00005
[11] Inoue, N., et al. (2020). Biomechanics of the Lumbar Facet Joint. DOI: 10.22603/SSRR.2019-0017
[12] Park, J. H., et al. (2025). Impact of asymmetric L4-L5 facet joint degeneration on lumbar spine biomechanics using a finite element approach. Scientific Reports. DOI: 10.1038/s41598-025-97021-3
[13] Du, C. F., et al. (2016). Biomechanical analysis of press-extension technique on degenerative lumbar with disc herniation and staggered facet joint. Journal of The Saudi Pharmaceutical Society. DOI: 10.1016/J.JSPS.2016.04.002
[14] Singh, D., et al. (2018). Lumbar hyperextension in baseball pitching: a potential cause of spondylolysis. Journal of Applied Biomechanics. DOI: 10.1123/JAB.2017-0230
[15] Cohen, S. P., et al. (2007). Pathogenesis, Diagnosis, and Treatment of Lumbar Zygapophysial (Facet) Joint Pain. Anesthesiology. DOI: 10.1097/00000542-200703000-00024
[16] Vora, A. J., et al. (2010). Functional anatomy and pathophysiology of axial low back pain: disc, posterior elements, sacroiliac joint, and associated pain generators. Physical Medicine and Rehabilitation Clinics of North America. DOI: 10.1016/J.PMR.2010.07.005
[17] Berven, S., et al. (2002). The lumbar zygapophyseal (facet) joints: a role in the pathogenesis of spinal pain syndromes and degenerative spondylolisthesis. Seminars in Neurology. DOI: 10.1055/S-2002-36542
[18] Jadon, A. (2016). Low Back Pain due to Lumbar Facet Joint Arthropathy and its Management. DOI: 10.4172/2327-5146.1000252
[19] Kleef, M., et al. Pain originating from the lumbar facet joints.
[20] Kozera, K., et al. (2017). Posterior Branches of Lumbar Spinal Nerves - part II: Lumbar Facet Syndrome - Pathomechanism, Symptomatology and Diagnostic Work-up. Ortopedia, Traumatologia, Rehabilitacja. DOI: 10.5604/15093492.1237716
[21] Vora, A. J., et al. (2010). Functional anatomy and pathophysiology of axial low back pain: disc, posterior elements, sacroiliac joint, and associated pain generators. Physical Medicine and Rehabilitation Clinics of North America. DOI: 10.1016/J.PMR.2010.07.005
[22] Beresford, Z. M., et al. (2010). Lumbar facet syndromes. Current Sports Medicine Reports. DOI: 10.1249/JSR.0B013E3181CABA05
[23] Garg, A., et al. (2017). Chronic Facet Pain. DOI: 10.1007/978-3-319-50512-1_94
[24] Susmarski, A., et al. (2017). Acute Facet Pain. DOI: 10.1007/978-3-319-50512-1_93
[25] Goetzinger, S. E., et al. (2020). Spondylolysis in Young Athletes: An Overview Emphasizing Nonoperative Management. Open Access Journal of Sports Medicine. DOI: 10.1155/2020/9235958
[26] Choi, E., et al. (2022). Management of lumbar spondylolysis in the adolescent athlete: a review of over 200 cases. The Spine Journal. DOI: 10.1016/j.spinee.2022.04.011
[27] Madden, C., et al. Spondylolysis: A Narrative Review of Etiology, Diagnosis, and Management.
[28] Standaert, C. J., et al. Spondylolysis. DOI: 10.1016/s1047-9651(18)30102-5
[29] Nau, E., et al. (2008). Spinal Conditioning for Athletes With Lumbar Spondylolysis and Spondylolisthesis. Strength and Conditioning Journal. DOI: 10.1519/SSC.0B013E31816A6D0F
[30] Mohile, N., et al. (2022). Spondylolysis and Isthmic Spondylolisthesis: A Guide to Diagnosis and Management. Journal of the American Board of Family Medicine. DOI: 10.3122/jabfm.2022.220130r1
[31] Selhorst, M., et al. (2020). Rehabilitation considerations for spondylolysis in the youth athlete. The International Journal of Sports Physical Therapy. DOI: 10.26603/IJSPT20200287
[32] Spondylolysis (2022). Orthopedic Reviews. DOI: 10.52965/001c.37470
[33] Metkar, U. S., et al. (2014). Conservative management of spondylolysis and spondylolisthesis. Seminars in Spine Surgery. DOI: 10.1053/J.SEMSS.2014.09.004
[34] Abdou, M., et al. (2025). Lumbar spinal stenosis: pathophysiology, biomechanics, and innovations in diagnosis and management. Journal of Spine Research and Surgery. DOI: 10.26502/fjsrs0082
[35] Adam, D., et al. (2011). Operative treatment of lumbar spinal stenosis with interspinous implants. General overview.
[36] Orita, S., et al. (2016). Lumbar foraminal stenosis, the hidden stenosis including at L5/S1. European Journal of Orthopaedic Surgery and Traumatology. DOI: 10.1007/S00590-016-1806-7
[37] Li, Y., et al. (2022). Spondylolisthesis. Orthopedic Reviews. DOI: 10.52965/001c.36917
[38] Lawrance, M., et al. (2022). CURRENT CLINICAL CONCEPTS: Management of Common Lumbar Spine Posterior Column Disorders. Journal of Athletic Training. DOI: 10.4085/1062-6050-0161.21
[39] Ball, J. R., et al. (2019). Lumbar Spine Injuries in Sports: Review of the Literature and Current Treatment Recommendations. Sports Medicine - Open. DOI: 10.1186/S40798-019-0199-7
[40] Spratt, K. F., et al. (1993). Efficacy of flexion and extension treatments incorporating braces for low-back pain patients with retrodisplacement, spondylolisthesis, or normal sagittal translation. Spine. DOI: 10.1097/00007632-199310000-00020
[41] Goetzinger, S. E., et al. (2020). Spondylolysis in Young Athletes: An Overview Emphasizing Nonoperative Management. Open Access Journal of Sports Medicine. DOI: 10.1155/2020/9235958
[42] Iwaki, T., et al. (2018). Physical features of pediatric patients with lumbar spondylolysis and effectiveness of rehabilitation. The Journal of Medical Investigation. DOI: 10.2152/JMI.65.177
[43] Parker, J., et al. MANAGEMENT OF LUMBAR SPONDYLOLYSIS IN THE ADOLESCENT ATHLETE USING A DYNAMIC NEUROMUSCULAR STABILIZATION PARADIGM: A Case Report.
[44] Muir, J. M. (2013). Conservative Physical Therapy Treatment for Posterolateral Derangement of the Lumbar Spine: A Case Report.
[45] The effectiveness of spinal manipulation versus spinal manipulation in conjunction with core stabilisation exercises in the treatment of mechanical low back pain (2022). DOI: 10.51415/10321/2103
[46] The relative effectiveness of manipulating the superior vertebral segment compared to manipulating the inferior vertebral segment in facet syndrome of the lumbar spine (2022). DOI: 10.51415/10321/2074
[47] Choi, E., et al. (2022). Management of lumbar spondylolysis in the adolescent athlete: a review of over 200 cases. The Spine Journal. DOI: 10.1016/j.spinee.2022.04.011
[48] Boyd, K., et al. (2018). Outcome of Conservative Management in the Treatment of Symptomatic Spondylolysis and Grade I Spondylolisthesis. Pediatrics. DOI: 10.1542/PEDS.142.1_MEETINGABSTRACT.329
[49] Metkar, U. S., et al. (2014). Conservative management of spondylolysis and spondylolisthesis. Seminars in Spine Surgery. DOI: 10.1053/J.SEMSS.2014.09.004
[50] Mazloum, V., et al. (2017). The effects of selective Pilates versus extension-based exercises on rehabilitation of low back pain. Journal of Bodywork and Movement Therapies. DOI: 10.1016/J.JBMT.2017.09.012
[51] Schwarz, A. (2008). Effectiveness of an extension-oriented treatment approach in a subgroup of subjects with low back pain: a randomized clinical trial. Manuelletherapie. DOI: 10.1055/S-2008-1027574
[52] Smith, B., et al. Comparing the Effectiveness of Extension-Based and Core Stability Exercises for Discogenic Lumbar Pathologies.
[53] Garet, M., et al. (2013). Nonoperative Treatment in Lumbar Spondylolysis and Spondylolisthesis A Systematic Review. Sports Health: A Multidisciplinary Approach. DOI: 10.1177/1941738113480936
[54] Haun, D. W., et al. (2005). Spondylolysis and spondylolisthesis: a narrative review of etiology, diagnosis, and conservative management. Journal of Chiropractic Medicine. DOI: 10.1016/S0899-3467(07)60153-0
[55] Carlson, B. B. (2007). Spondylolysis and the Athlete. Athletic Therapy Today. DOI: 10.1123/ATT.12.4.37
[56] Purcell, L. (2009). Causes and prevention of low back pain in young athletes. Paediatrics and Child Health. DOI: 10.1093/PCH/14.8.533
[57] Vad, V. B., et al. (2003). Role of radiofrequency denervation in lumbar zygapophyseal joint synovitis in baseball pitchers: a clinical experience. Pain Physician. DOI: 10.36076/PPJ.2003/6/307
[58] Nau, E., et al. (2008). Spinal Conditioning for Athletes With Lumbar Spondylolysis and Spondylolisthesis. Strength and Conditioning Journal. DOI: 10.1519/SSC.0B013E31816A6D0F
ごあいさつ

長引いた痛みを一人で治すのは困難なことが多いです。
困ったときは自身で判断せずに適切な処置を受けるために専門家に相談しましょう。
もし、お近くにお住まいで、困っているならば、一度ひまわり接骨院までお問い合わせください。腰痛・坐骨神経痛の専門家の新幡が、ご相談に乗ります。
気軽にご相談ください。

新着情報・お知らせ
平常通り営業致します。
4・5・6は祝日の為、お休みになります。
29(水)は祝日の為、お休みになります。
お気軽にお問合せください

お電話でのお問合せ・相談予約
<受付時間>
月~土
9:00〜13:00 /15:00〜19:00
※日曜・祝日は除く
フォームは24時間受付中です。お気軽にご連絡ください。
- トップページ
ひまわり接骨院

住所
〒213-0002
神奈川県川崎市高津区二子1丁目7−17 リバーサイドマンション杉崎 102
アクセス
二子新地駅 徒歩3分
駐車場:近隣にコインパーキングあり。自転車・バイクは店舗前に駐輪場がございます。
受付時間
月~土
9:00〜13:00 /15:00〜19:00
定休日
日曜・祝日

