
〒213-0002 神奈川県川崎市高津区二子1丁目7−17
リバーサイドマンション杉崎 102 二子新地駅 徒歩3分
| 月 | 火 | 水 | 木 | 金 | 土 | 日祝 | |
|---|---|---|---|---|---|---|---|
| 9:00〜13:00 | ● | ● | ● | ● | ● | ● | ─ |
| 15:00〜19:00 | ● | ● | ● | ● | ● | ● | ─ |
腰椎椎間板ヘルニアの重症度を決めるのは?
公開日:2026/06/04
更新日:2026/00/00
腰部椎間板ヘルニア(LDH)の重症度や予後を予測する因子について、最新のエビデンスに基づき解説した包括的なガイドです。
報告書は、MRI画像による解剖学的特徴、心理社会的側面、炎症マーカー、そして生活習慣という多角的な視点から、再発リスクや治療の経過に影響を与える要素を整理しています。
特に髄核突出やModic変化といった構造的要因に加え、喫煙や肥満、糖尿病が術後の再発に強く関与することを強調しています。
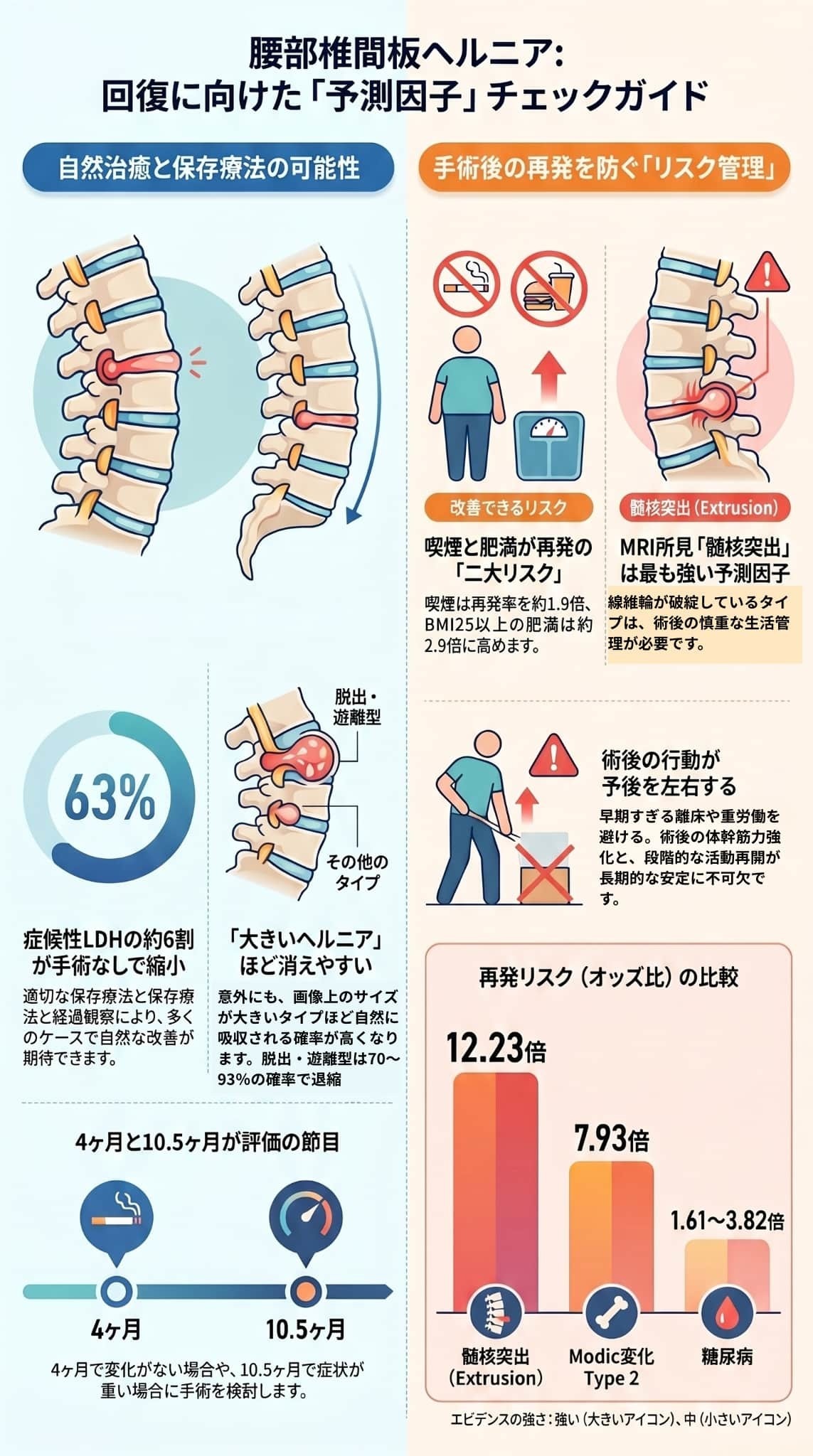
一方で、手術をしない保存療法でも約63%の患者でヘルニアが自然退縮するというデータを示し、適切な治療選択の基準を提示しています。
最終的に、患者が自ら改善できる禁煙や体重管理の重要性を説き、医療者と対話しながら個別化された治療計画を立てるための具体的な指針をまとめています。
目次
腰部椎間板ヘルニア(LDH)の重症度や予後に影響を与える予測因子は、主に「生体力学的・解剖学的因子」「生活習慣・行動因子」「臨床的因子」「生物学的因子」の4つの側面に分類して整理されています。2016年以降の高品質な研究に基づく主要な知見は以下の通りです。
- 髄核突出(Extrusion): 椎間板の線維輪が破れ、髄核が脊柱管内に突出した状態です。手術後の再発リスクを約12倍(オッズ比12.23)に高める、最も強力な予測因子とされています。
- Modic変化 Type 2: 椎体終板周囲の炎症や脂肪化を示す所見であり、椎間板の治癒能力低下を反映するため、再発リスクを約7.9倍高めます。
- 大きな環状欠損: 手術の際にできる線維輪の開口部が大きいほど、術後の力学的弱点となって再突出(再発)のリスクが高まります(オッズ比2.19)。
- 喫煙: LDHの発症リスクを高めるだけでなく、手術後の再発リスクを約1.4〜1.9倍、再手術リスクを増加させる確立されたリスク因子です。禁煙は、再発を防ぐための「第1優先」の行動指針とされています。
- 肥満(高BMI): BMI25以上の肥満は、椎間板への機械的負荷の増加や慢性炎症を通じて、発症リスク(オッズ比2.77)と再発リスクを有意に高めます。段階的な体重減少が推奨されています。
- 職業的負荷: 前屈姿勢や重量物の取り扱いは発症リスクを1.6〜3.7倍に増加させます。
- 高齢(60歳以上): 組織の治癒能力の低下や併存疾患の影響により、手術後の再発リスク(オッズ比2.23)や機能障害が高まることが示されています。
- 糖尿病: 組織治癒能力の低下や微小血管障害を引き起こし、術後の再発リスクを約1.6〜3.8倍に高めます。予後改善には適切な血糖コントロールが不可欠です。
- 性別(女性): 再発リスク自体に男女差はないものの、女性は術後の持続的な痛みや復職困難のリスクが相対的に高い傾向にあります。
- 大きなヘルニアほど自然に縮小しやすい: 手術をしない保存療法を選んだ場合、症候性患者の約63%でヘルニアが自然に縮小(退縮)します。特筆すべき点として、「脱出型」や「遊離型」といったサイズの大きなヘルニアであるほど退縮率が高く(70〜93%)、重度の神経障害がない限りは保存療法をまず試みることが推奨されます。
- 炎症の二面性: ヘルニア周囲の炎症(サイトカインなど)は痛みの原因である一方で、マクロファージなどがヘルニア組織を吸収して自然退縮を促進する重要な働きを持っています。そのため、急性期の過度な抗炎症治療はかえって治癒を妨げる可能性があります。
腰椎椎間板ヘルニアHの予後は髄核突出やModic変化といった「変えられない構造的因子」に強く影響されますが、「喫煙」「肥満」「糖尿病」といった改善可能な因子に積極的に介入することで、再発リスクを大幅に下げることができます。医療者と情報を共有し、これらの因子に基づく個別化されたリスク評価を行うことが、最良の治療選択に繋がります。
腰部椎間板ヘルニア(LDH)の重症度や予後を予測する「生体力学的・解剖学的因子」は、主にMRIやX線検査で確認できる椎間板や脊椎の構造的特徴を指します。これらは特に手術後の再発リスクに強く影響を与えます。最新のシステマティックレビューに基づく主な因子は以下の通りです。
- エビデンスの強さ:強い
- 再発リスク: 髄核突出がある場合、ない場合と比較して**再発リスクが約12倍(オッズ比12.23)**と、最も強力な予測因子です。
- 特徴: 椎間板の線維輪が完全に破れ、内部の髄核組織が靭帯を越えて脊柱管内に飛び出した状態です。この構造的な不安定性により、手術後も同じ場所から再びヘルニアが突出するリスクが高くなります。
- 対策: MRIで「突出(extrusion)」と診断された場合は、術後の重量物の持ち上げ制限や体重管理など、生活習慣の管理が極めて重要になります。
- エビデンスの強さ:強い
- 再発リスク: Modic変化Type 2がある患者の**再発リスクは約7.9倍(オッズ比7.93)**です。
- 特徴: 椎体終板(椎間板と骨の境界)周囲の骨髄が脂肪に置き換わるなどの変化を示すMRI所見であり、椎間板の治癒能力低下や局所的な炎症を反映しています。
- 年齢による違い: 50.5歳未満の若年患者では再発の非常に強い予測因子(オッズ比14.27)になりますが、高齢患者では椎間板変性が全体的に進行しているため、この所見単独の相対的な影響は小さくなります。
- エビデンスの強さ:中〜強
- 再発リスク: 大きな環状欠損がある場合、再発リスクは約2.2倍(オッズ比2.19)です。
- 特徴: 手術の際に髄核を取り出すために作られる線維輪の開口部のことです。この欠損(穴)が大きいほど、術後の力学的な弱点となり、残った髄核が再突出するリスクが高まります。
- エビデンスの強さ:中
- 特徴: これらは背骨の「グラつき(セグメント不安定性)」を示す指標です。椎間板の高さが保たれすぎている場合や、前後に動かしたときの可動域が大きい場合は、力学的に不安定であり、術後の再発リスクを高める可能性があります。
- 年齢による違い: 高齢患者(50.5歳以上)においては、椎間板高さ指標の増加が再発の有意な予測因子になることが示されています。術後の体幹筋力強化や姿勢管理が推奨されます。
- エビデンスの強さ:中〜矛盾あり
- 特徴: 椎間板の変性具合を5段階で評価する指標ですが、再発との関連については研究によって結果が分かれています。全体としては明確な関連がないものの、内視鏡手術(PELD)後に限定すると、変性が強い(グレード4以上)場合は再発リスクが約2.8倍高まると報告されています。
- エビデンスの強さ:弱〜中
- 特徴: 背骨の後ろ側にある左右の「椎間関節」の向きが非対称である状態を指します。これは生まれつきの構造的特徴であり、椎間板に不均等なストレスをかけるため、ヘルニアの発生や再発(オッズ比1.465)に関与する可能性があります。
生体力学的・解剖学的因子の中で、特に**「髄核突出」と「Modic変化 Type 2」**は手術後の再発を予測する非常に強力な因子です。
これらの構造的な特徴自体は患者自身の努力で変えることはできませんが、自身のリスクを正確に把握することで、術後のより慎重な生活習慣の管理やリハビリテーションに活かすことができます。
腰部椎間板ヘルニア(LDH)の重症度や手術後の予後に影響を与える心理社会的・臨床的因子には、以下のようなものがあります。構造的な要因だけでなく、患者の年齢や持病、心理状態も長期的な回復に大きく関与します。
高齢患者は椎間板の治癒能力の低下や併存疾患の増加などにより、手術後の再発リスクが上昇(オッズ比2.23)し、機能障害が大きくなることが示されています。年齢が10歳増加するごとに、機能障害を測る指標(Oswestry Disability Index)が1.47点悪化するという報告もあります。
女性であること自体は再発リスクを有意に高めるわけではありませんが、術後の持続的な脚の痛みや、復職困難(オッズ比2.79)、うつ病状態の高いリスクと関連しています。そのため、女性患者においては疼痛管理や心理的サポート、職場復帰支援など包括的なケアがより重要になります。
糖尿病は、組織の治癒能力を低下させたり微小血管障害を引き起こしたりすることで、術後の再発リスクを約1.6〜3.8倍(オッズ比1.61〜3.82)に高めることが複数の研究で示されています。術前・術後における適切な血糖コントロールが、再発リスクを下げるために非常に重要です。
症状が長期間(4年以上など)続いている場合、再発リスクの上昇(オッズ比2.93)や、うつ・不安といった心理的ストレス増大の独立したリスク因子になることが報告されています。一方で、発症から1年以内の早期手術が、より早い回復と良好な結果をもたらす可能性も示唆されています。
腰部椎間板ヘルニア(LDH)の予後や重症度予測において、通常のMRIによる構造評価だけでなく、特定の画像所見や分子・遺伝レベルの因子も影響を与えることが明らかになってきています。主な知見は以下の通りです。
- High Intensity Zone (HIZ): T2強調MRI画像で椎間板の後方線維輪に見られる高信号領域のことで、線維輪の亀裂や炎症を反映します。HIZがある場合、痛みの再現と強い関連(オッズ比8.65)があるほか、特定の治療(経皮的硬膜外癒着剥離術など)においては術後の治療反応を予測する因子になる可能性があります。ただし無症状の人にも見られるため、これ単独で痛みの原因とは断定できません。
- 定量的MRI指標(T2緩和時間): 椎間板の水分含有量や組織構造を定量的に評価する技術です。初期の髄核T2値などを測定することで、将来のヘルニア発生や数年後の痛み・機能障害を高い精度で予測できる可能性が示されています。
- 痛みを増強する炎症促進性サイトカイン(M1系): TNF-αやIL-6などの数値が高い状態は炎症反応が活発であることを示し、強い痛み(高いVASスコア)や持続的な神経根痛と関連することが報告されています。
- 修復を促す抗炎症性サイトカイン(M2系): 一方で、IL-4やIL-10といったマーカーが高い場合は、炎症が収束に向かい組織修復が促進されていることを示し、痛みが軽いことと関連しています。
- 炎症の「二面性」と自然退縮: マクロファージなどによる炎症反応は痛みの原因となる一方で、ヘルニア組織を吸収し自然退縮(自然治癒)を促進するために不可欠な役割を担っています。そのため、急性期に過度な抗炎症治療を行うと、かえって治癒を妨げてしまう可能性があります。
- 遺伝子多型(SNV): アグリカン(ACAN)遺伝子の変異がLDHの重症度と関連していることや、特定の遺伝子変異(OPRM1、COMTなど)が腰部神経根痛からの回復低下と関連することが報告されています。
- 大規模なゲノム解析でもLDHと関連する数十の遺伝子座が同定されており、遺伝的な感受性が発症リスクや重症度に影響を与える可能性が示唆されています。
これらの画像所見や生物学的・遺伝的因子は、将来的に血液検査や遺伝子検査を通じた個別のリスク評価や治療計画(個別化医療)に役立つと期待されています。
しかし、大部分は現時点では研究段階であり、一般的な臨床検査としては確立されていません。そのため現段階ではこれらの因子に過度な期待を持たず、先述したようなエビデンスの強い構造的因子(髄核突出など)への対処や、改善可能な生活習慣(禁煙、体重管理など)の改善を優先することが重要視されています。
腰部椎間板ヘルニア(LDH)の重症度や予後を予測する「生活習慣・行動因子」は、構造的因子(ヘルニアの形や大きさなど)とは異なり、**患者自身が自ら介入して改善できる(可変的である)**という点で、予後を良くするための極めて重要な領域です。
- エビデンスの強さ:強い
- 影響: 喫煙はLDHの発症リスクを高めるだけでなく、手術後の再発リスクを約1.8倍(オッズ比1.80〜1.87)、再手術リスクを約1.4倍増加させる、最も確立されたリスク因子の一つです。
- メカニズム: 喫煙による微小血管障害が椎間板への栄養供給を低下させ、組織の治癒能力を阻害し、炎症反応を増強させることで、椎間板の変性を促進します。
- 対策: 手術前から禁煙を開始するのが理想ですが、手術後に禁煙を始めても長期的な予後改善が期待できます。患者自身ができる行動の中で、最も効果的な「第1優先」の指針とされています。
- エビデンスの強さ:中〜強
- 影響: BMIが25以上の肥満は、**発症リスクを約2.8倍(オッズ比2.77)高め、手術後の再発リスクも大きく増加(オッズ比2.89)**させます。BMIが1ポイント増加するごとに、再発リスクが1.23倍高まるという報告もあります。
- メカニズム: 体重増加による椎間板への直接的な機械的負荷の増大に加えて、肥満が引き起こす全身の慢性炎症状態が、組織の治癒能力を低下させます。
- 対策: 急激な減量ではなく、適度な運動と栄養管理による**段階的な体重減少(月に1〜2kg)**が推奨されており、BMIがわずかに下がるだけでも再発リスクの低減に繋がる可能性があります。
- エビデンスの強さ:中
- 影響: 前屈姿勢や重量物の取り扱いといった腰部への累積的な負荷は、発症リスクを1.6倍から3.7倍に増加させます。ただし、手術後の「再発」との関連については研究間で結果が一致していません。
- 対策: 術後早期の重労働は避け、職場復帰の際は適切な持ち上げ技術の習得や、持ち上げ補助具の導入など、環境の改善と段階的な負荷の増加が重要です。
- エビデンスの強さ:不十分(限定的)
- 影響: 長時間の座位と中〜高強度の身体活動の組み合わせや、過度なスポーツ参加(週4〜5回)が発症リスクを高める可能性が指摘されています。また興味深い点として、手術後の「離床時期」が早すぎる(平均17日 vs 24日)と、かえって再発群に多かったという報告もあり、過度な活動再開には注意が必要です。
- 対策: 長時間の同一姿勢を避けることと、術後は過度な安静や急激な活動再開を避け、理学療法士などの指導のもとで適度な活動と体幹筋力強化を行うことが推奨されます。
腰部椎間板ヘルニア(LDH)の治療において、「保存療法(手術をしない治療)」と「手術療法」のどちらを選択するかは、患者と医療者にとって非常に重要な決断です。この2つの治療法は、予後を左右する要因(予測因子)が全く異なるという特徴を持っています。
重度の神経障害(明らかな筋力低下など)や排尿・排便障害がない限り、まずは保存療法が推奨されます。
- 「大きなヘルニア」ほど治りやすい(強いエビデンス): 保存療法を選んだ場合、全体の約63%でヘルニアが自然に縮小(退縮)します。驚くべきことに、ヘルニアのサイズが大きいほど退縮率が高く、膨隆型(13.3%)や突出型(52.5%)よりも、靭帯を突き破った**「脱出型(70.4%)」や完全に分離した「遊離型(93.0%)」の方が、極めて高い確率で自然縮小**します。
- 予測の限界: 一方で、「どの患者の保存療法が確実に成功するか」を事前に見分けるための決定的な予測因子は、現時点では確立されていません。そのため、治療効果には個人差が大きいという前提を理解する必要があります。
- 推奨される評価スケジュール: 保存療法を続ける場合は、**「発症後4か月」と「約10.5か月」**での再評価が推奨されています。4か月時点でMRI上の退縮が見られない場合や、10.5か月時点で重度の症状が残っている場合に、手術への切り替えを検討します。
手術は早期の痛みの改善に有効ですが、平均13.1%の再発リスクや、感染などの合併症リスクを伴います。手術後の予後は、構造的な問題と患者自身の生活習慣に強く依存します。
■改善不可能な構造的因子(強いエビデンス):
- 髄核突出(Extrusion):再発リスクが約12倍(オッズ比12.23)。
- Modic変化 Type 2(椎体の脂肪化):再発リスクが約7.9倍(オッズ比7.93)。
- 大きな環状欠損(手術時の線維輪の穴):再発リスクが約2.2倍。
- これらがある患者は、術後の再発リスクが必然的に高くなるため、術後のより慎重な生活指導(重量物の持ち上げ制限など)が必要です。
■改善可能な生活習慣・併存疾患因子(強いエビデンス):
- 喫煙、肥満(高BMI)、糖尿病は、いずれも術後の再発や再手術のリスクを約1.4倍〜3.8倍に引き上げる強力な予測因子です。これらは患者自身の努力と治療で変えることができるため、手術を選択する際のリスク管理の要となります。
■機能回復を阻害する因子:
- 高齢(60歳以上)や、女性(復職困難のリスクが高い)、術前の医療用麻薬(オピオイド)の使用などは、術後の痛みの持続や機能障害(生活の質の低下)と関連します。該当する場合は、理学療法や心理的サポートを含めた手厚い術後ケアが必要です。
- 保存療法の成功は、患者の持つ**「自然治癒力(マクロファージ等によるヘルニアの吸収)」**に依存しています。「MRIでヘルニアが大きいと言われたから手術しかない」というのは誤解であり、むしろ大きなヘルニア(脱出型・遊離型)ほど自然退縮を期待して保存療法を粘り強く試みる価値があります。
- 手術療法の成功は、構造的リスクを理解した上での**「自己管理(ライフスタイルの改善)」**に依存しています。手術をすれば全て完治するわけではなく、喫煙や肥満、糖尿病を放置したままでは再発の危険性が非常に高くなります。
これらの違いをふまえ、医療者と「自分自身のヘルニアのタイプは自然退縮しやすいか」「自分には手術後に再発しやすいリスク(喫煙や肥満など)があるか」を話し合い、納得のいく治療法を選択することが最も重要です。
腰部椎間板ヘルニア(LDH)の患者教育における実践的提言と行動指針は、患者自身が「変えられないリスク」に圧倒されることなく、「改善可能な因子」に焦点を当てて具体的な行動を起こせるよう導くことを目的としています。
■第1優先:禁煙
- 理由: 喫煙は手術後の再発リスクを約1.4〜1.9倍に高める、最も確立されたリスク因子です。
- 行動指針: 禁煙外来の利用や禁煙補助薬(ニコチン置換療法など)について担当医と相談し、家族のサポートを得ることが推奨されます。手術前から始めるのが理想ですが、手術後に開始しても長期的な予後改善が期待できるため、いつでも遅すぎることはありません。
■第2優先:段階的な体重管理
- 理由: BMI25以上の肥満は、発症リスク(2.77倍)および再発リスク(2.89倍)を有意に高めます。
- 行動指針: 急激な減量ではなく、月に1〜2kgの段階的な体重減少を目標とします。適度な運動(ウォーキングや水泳など)を取り入れ、必要に応じて栄養士の指導を受けることが推奨されます。
■第3優先:併存症の管理と職業的負荷の軽減
- 糖尿病管理: 糖尿病は再発リスクを1.6〜3.8倍に高めるため、術前・術後を通じた定期的な血糖測定とコントロールが不可欠です。
- 職業的負荷: 重量物の持ち上げや前屈姿勢は発症リスクを増加させます。職場環境の改善(持ち上げ補助具の導入など)を雇用主と相談し、術後早期の重労働は避けるべきです。
- 画像診断の理解: MRIで「髄核突出(extrusion)」や「Modic変化 Type 2」と言われた場合、再発リスクが非常に高いため、より慎重な術後管理が必要です。
- 治療歴や背景: 術前のオピオイド(医療用麻薬)の使用や、労災補償などの法的問題が絡んでいる場合、術後の痛みの管理や回復に悪影響を及ぼす可能性があるため、必ず申告します。
- 心理的状態: うつ、不安、痛みに対する過度な恐怖(恐怖回避)や破局的思考は、痛みの悪化と関連するため、これらの精神的ストレスも医療者と共有します。
- 保存療法を優先する: 重度の神経障害(筋力低下など)や膀胱直腸障害がない限り、まずは保存療法を優先します。患者の約63%でヘルニアは自然に縮小し、特にサイズの大きなヘルニア(脱出型・遊離型)ほど7〜9割の高確率で退縮します。
- 手術を選ぶ場合のリスク管理: 手術は平均13.1%の再発リスクなどを伴います。手術を成功させるには、前述の「禁煙」「体重管理」「血糖コントロール」に加えて、術後の重量物持ち上げ制限や、早すぎない適切な離床時期の遵守など、徹底した自己管理が鍵となります。
- 保存療法のタイムライン: 保存療法を続ける場合、発症後「4か月」と「約10.5か月」のタイミングで再評価を行うことが推奨されています。
- 記録をつける: 痛みの強さ(VASスコア)、日常生活の制限度、神経症状(感覚障害など)、心理状態を日々記録し、医療者に報告することで、的確な治療方針の修正が可能になります。
患者教育における最も重要なメッセージは、椎間板ヘルニアの予後は決して「運命」ではなく、患者自身が生活習慣を改善することで結果を大きく好転させることができるという点です。エビデンスの強い因子(禁煙、減量など)に的を絞って具体的な一歩を踏み出し、医療者と密に連携(エンパワーメント)することが、最良の回復への道筋となります。
[1]L. Mendonça, M. Monteiro-Soares, and L. F. Azevedo, “Prediction of Clinical Outcomes in Individuals With Chronic Low Back Pain: A Protocol for a Systematic Review With Meta-Analysis,” Systematic Reviews, vol. 7, no. 1, pp. 149–149, Oct. 2018, doi: 10.1186/S13643-018-0818-2.
[2]E. M. Pinto, J. Rocha-Neves, and M. Laranjeira, “The importance of inflammatory biomarkers in non-specific acute and chronic low back pain: a systematic review.,” European Spine Journal, May 2023, doi: 10.1007/s00586-023-07717-1.
[3]W. Mika, J. Moszkowicz, J. Słowik, D. Narożniak, M. Mierniczek, and A. Rodzeń, “Prognostic factors in low back pain: from identification to stratified care,” Archiv EuroMedica, vol. 15, no. 5, Oct. 2025, doi: 10.35630/2025/15/iss.5.515.
[4]C. A, W. R., O. C., C. T, H. Ca, and L. J, “Theoretical Schemas to Guide Back Pain Consortium (BACPAC) Chronic Low Back Pain Clinical Research,” Sept. 2025, doi: 10.7302/27327.
[5]A. Chau et al., “Theoretical Schemas to Guide BACPAC Chronic Low Back Pain Clinical Research.,” Pain Medicine, Dec. 2022, doi: 10.1093/pm/pnac196.
[6]E. Otero-Ketterer, C. Peñacoba-Puente, C. F. Pinheiro-Araujo, J. A. Valera-Calero, and R. Ortega-Santiago, “Biopsychosocial Factors for Chronicity in Individuals with Non-Specific Low Back Pain: An Umbrella Review,” International Journal of Environmental Research and Public Health, vol. 19, no. 16, pp. 10145–10145, Aug. 2022, doi: 10.3390/ijerph191610145.
[7]S. G. Hassan, K. Nesovic, J. Babineau, A. D. Furlan, D. Kumbhare, and L. C. Carlesso, “Identifying chronic low back pain phenotypic domains and characteristics accounting for individual variation: a systematic review.,” Pain, vol. Publish Ahead of Print, Apr. 2023, doi: 10.1097/j.pain.0000000000002911.
[8]J. Boissoneault, J. M. Mundt, M. E. Robinson, and S. Z. George, “Predicting Low Back Pain Outcomes: Suggestions for Future Directions,” Journal of Orthopaedic & Sports Physical Therapy, vol. 47, no. 9, pp. 588–592, Aug. 2017, doi: 10.2519/JOSPT.2017.0607.
[9]N. AUTHOR_ID, N. AUTHOR_ID, and A. M. Elabd, “Prediction of Back Disability Using Clinical, Functional, and Biomechanical Variables in Adults with Chronic Nonspecific Low Back Pain,” Stomatology, vol. 13, no. 13, pp. 3980–3980, July 2024, doi: 10.3390/jcm13133980.
[10]“Spinal degeneration and lumbar multifidus muscle quality may independently affect clinical outcomes in patients conservatively managed for low back or leg pain,” Dental science reports, vol. 14, no. 1, Apr. 2024, doi: 10.1038/s41598-024-60570-0.
[11]R. K. Jensen, P. Kent, T. S. Jensen, and P. Kjaer, “The association between subgroups of MRI findings identified with latent class analysis and low back pain in 40-year-old Danes.,” BMC Musculoskeletal Disorders, vol. 19, no. 1, pp. 62–62, Feb. 2018, doi: 10.1186/S12891-018-1978-X.
[12]J. J. Wong et al., “Association Between Depressive Symptoms or Depression and Health Outcomes for Low Back Pain: a Systematic Review and Meta-analysis.,” Journal of General Internal Medicine, pp. 1–14, Aug. 2021, doi: 10.1007/S11606-021-07079-8.
[13]A. Alhowimel, A. Alhowimel, M. Alotaibi, M. Alotaibi, K. Radford, and N. S. Coulson, “Psychosocial factors associated with change in pain and disability outcomes in chronic low back pain patients treated by physiotherapist: A systematic review.,” Sage Open Medicine, vol. 6, pp. 2050312118757387–2050312118757387, Feb. 2018, doi: 10.1177/2050312118757387.
[14]A. S. Alhowimel et al., “Psychosocial Predictors of Pain and Disability Outcomes in People with Chronic Low Back Pain Treated Conservatively by Guideline-Based Intervention: A Systematic Review”, doi: 10.2147/jmdh.s343494.
[15]G. Buruck, A. Tomaschek, J. Wendsche, E. Ochsmann, and D. Dörfel, “Psychosocial areas of worklife and chronic low back pain: a systematic review and meta-analysis,” BMC Musculoskeletal Disorders, vol. 20, no. 1, pp. 480–480, Oct. 2019, doi: 10.1186/S12891-019-2826-3.
[16]S. Vickery et al., “Integrating multidimensional data analytics for precision diagnosis of chronic low back pain,” medRxiv, vol. 15, Oct. 2024, doi: 10.1038/s41598-025-93106-1.
[17]I. Løchting et al., “The impact of psychological factors on condition-specific, generic and individualized patient reported outcomes in low back pain,” Health and Quality of Life Outcomes, vol. 15, no. 1, p. 40, Feb. 2017, doi: 10.1186/S12955-017-0593-0.
[18]D. C. Felício et al., “Risk factors for non-specific low back pain in older people: a systematic review with meta-analysis.,” Archives of Orthopaedic and Trauma Surgery, pp. 1–10, May 2021, doi: 10.1007/S00402-021-03959-0.
[19]Elgaeva et al., “Bidirectional Mendelian Randomization Study of Personality Traits Reveals a Positive Feedback Loop Between Neuroticism and Back Pain.,” The journal of pain, 2023, doi: 10.1016/j.jpain.2023.05.012.
[20]P. Suri, M. Kazemi-Naini, and F. Williams, “The Association Between Individual Lumbar Intervertebral Disc Degeneration Features and Low Back Pain is Modified by Genetic Propensity to Pain,” The Journal of Pain, Apr. 2024, doi: 10.1016/j.jpain.2024.01.209.
[21]R. S. Perera, “Role of lumbar disc degeneration and genetic variation in chronic low back pain,” Ceylon Journal of Medical Science, vol. 55, no. 1, p. 3, Aug. 2018, doi: 10.4038/CJMS.V55I1.4931.
[22]“Nonspecific Low Back Pain,” The New England Journal of Medicine, vol. 386, no. 18, pp. 1732–1740, May 2022, doi: 10.1056/nejmcp2032396.
[23]P. K. Morris, K. Ali, M. Merritt, J. Pelletier, and L. G. Macedo, “A systematic review of the role of inflammatory biomarkers in acute, subacute and chronic non-specific low back pain.,” BMC Musculoskeletal Disorders, vol. 21, no. 1, pp. 1–12, Mar. 2020, doi: 10.1186/S12891-020-3154-3.
[24]V. T. Enrico et al., “Plasma Pro‐ and Anti‐Inflammatory Cytokines in an Observational Chronic Low Back Pain Cohort,” JOR spine, vol. 8, no. 3, Sept. 2025, doi: 10.1002/jsp2.70095.
[25]M. D. Vigeland et al., “Gene Expression Correlates with Disability and Pain Intensity in Patients with Chronic Low Back Pain and Modic Changes in a Sex-Specific Manner,” International Journal of Molecular Sciences, vol. 26, no. 2, pp. 800–800, Jan. 2025, doi: 10.3390/ijms26020800.
[26]R. Compte, M. K. Naeini, E. Heikkala, T. McSweeney, J. Karppinen, and F. M. K. Williams, “Does combining the STarT Back Tool with a polygenic risk score for chronic low back pain improve prediction of work disability over two years?,” Sept. 2025, doi: 10.1101/2025.09.09.25335394.
[27]P. Suri et al., “Genome-wide meta-analysis of 158,000 individuals of European ancestry identifies three loci associated with chronic back pain.,” PLOS Genetics, vol. 14, no. 9, pp. 1–23, Sept. 2018, doi: 10.1371/JOURNAL.PGEN.1007601.
[28]M. C. Brown et al., “Patterns and trajectories of peripheral inflammatory cytokines, immune tolerance, and lymphocyte differentiation predict transition from acute to chronic low back pain in a sex- and age-specific manner,” Pain, Oct. 2025, doi: 10.1097/j.pain.0000000000003811.
[29]Y. Z. Lim et al., “Association Between Inflammatory Biomarkers and Nonspecific Low Back Pain: A Systematic Review.,” The Clinical Journal of Pain, vol. 36, no. 5, pp. 379–389, Jan. 2020, doi: 10.1097/AJP.0000000000000810.
[30]P. Suri et al., “Genome-wide Meta-analysis of 158,000 Individuals of European Ancestry Identifies Three Loci Associated with Chronic Back Pain,” bioRxiv, p. 244483, Jan. 2018, doi: 10.1101/244483.
[31]K. Verkerk, P. A. J. Luijsterburg, H. S. Miedema, A. Pool-Goudzwaard, and B. W. Koes, “Prognostic Factors for Recovery in Chronic Nonspecific Low Back Pain: A Systematic Review,” Physical Therapy, vol. 92, no. 9, pp. 1093–1108, Sept. 2012, doi: 10.2522/PTJ.20110388.
[32]S. S. Sribastav et al., “Risk Factors Associated with Pain Severity in Patients with Non-specific Low Back Pain in Southern China.,” Asian Spine Journal, vol. 12, no. 3, pp. 533–543, June 2018, doi: 10.4184/ASJ.2018.12.3.533.
[33]I. M. da C. Fernandes, R. Z. Pinto, P. H. Ferreira, and F. S. Lira, “Low back pain, obesity, and inflammatory markers: exercise as potential treatment,” Journal of exercise rehabilitation, vol. 14, no. 2, pp. 168–174, Apr. 2018, doi: 10.12965/JER.1836070.035.
[34]Silva, Hayden, Mendes, Verhagen, Pinto, and Silva, “Sleep as a prognostic factor in low back pain: a systematic review of prospective cohort studies and secondary analyses of randomized controlled trials.,” Sleep, 2024, doi: 10.1093/sleep/zsae023.
[35]D. N. K, G. E. J, V. A. M, T. S. S, and H. A. C, “Prognostic Factors for Disability and Pain Outcomes in Patients with Axial Low Back Pain Undergoing a Multidisciplinary Spine Treatment Program,” vol. 6, no. 1, Jan. 2020, doi: 10.23937/2572-4215.1510019.
[36]F. Russo et al., “Prognostic factors for return to work in patients affected by chronic low back pain: a systematic review,” Musculoskeletal Surgery, June 2024, doi: 10.1007/s12306-024-00828-y.
[37]B. N. Green et al., “A scoping review of biopsychosocial risk factors and co-morbidities for common spinal disorders,” PLOS ONE, vol. 13, no. 6, p. 0197987, June 2018, doi: 10.1371/JOURNAL.PONE.0197987.
[38]J. Yang, W. L. A. Lo, F. Zheng, X. Cheng, Q. Yu, and C. Wang, “Evaluation of Cognitive Behavioral Therapy on Improving Pain, Fear Avoidance, and Self-Efficacy in Patients with Chronic Low Back Pain: A Systematic Review and Meta-Analysis,” Pain Research & Management, vol. 2022, pp. 1–15, Mar. 2022, doi: 10.1155/2022/4276175.
[39]E. K. Ho et al., “Psychological interventions for chronic, non-specific low back pain: systematic review with network meta-analysis,” BMJ, vol. 376, pp. e067718–e067718, Mar. 2022, doi: 10.1136/bmj-2021-067718.
[40]A. C. Traeger et al., “Estimating the Risk of Chronic Pain: Development and Validation of a Prognostic Model (PICKUP) for Patients with Acute Low Back Pain,” PLOS Medicine, vol. 13, no. 5, pp. 1–21, May 2016, doi: 10.1371/JOURNAL.PMED.1002019.
[41]E. L. Karran et al., “Can screening instruments accurately determine poor outcome risk in adults with recent onset low back pain? A systematic review and meta-analysis.,” BMC Medicine, vol. 15, no. 1, pp. 13–13, Jan. 2017, doi: 10.1186/S12916-016-0774-4.
ごあいさつ

長引いた痛みを一人で治すのは困難なことが多いです。
困ったときは自身で判断せずに適切な処置を受けるために専門家に相談しましょう。
もし、お近くにお住まいで、困っているならば、一度ひまわり接骨院までお問い合わせください。腰痛・坐骨神経痛の専門家の新幡が、ご相談に乗ります。
気軽にご相談ください。

新着情報・お知らせ
平常通り営業致します。
4・5・6は祝日の為、お休みになります。
お気軽にお問合せください

お電話でのお問合せ・相談予約
<受付時間>
月~土
9:00〜13:00 /15:00〜19:00
※日曜・祝日は除く
フォームは24時間受付中です。お気軽にご連絡ください。
- トップページ
ひまわり接骨院

住所
〒213-0002
神奈川県川崎市高津区二子1丁目7−17 リバーサイドマンション杉崎 102
アクセス
二子新地駅 徒歩3分
駐車場:近隣にコインパーキングあり。自転車・バイクは店舗前に駐輪場がございます。
受付時間
月~土
9:00〜13:00 /15:00〜19:00
定休日
日曜・祝日

