
〒213-0002 神奈川県川崎市高津区二子1丁目7−17
リバーサイドマンション杉崎 102 二子新地駅 徒歩3分
| 月 | 火 | 水 | 木 | 金 | 土 | 日祝 | |
|---|---|---|---|---|---|---|---|
| 9:00〜13:00 | ● | ● | ● | ● | ● | ● | ─ |
| 15:00〜19:00 | ● | ● | ● | ● | ● | ● | ─ |
マインドフルネス・ストレス低減法による腰痛治療
公開日:2026/03/30
更新日:2026/06/10
慢性腰痛に対するマインドフルネス・ストレス低減法(MBSR)の有効性を検証した膨大な学術論文や臨床試験の結果をまとめたリサーチレビューです。
研究データによると、MBSRは痛みの緩和や身体機能の改善だけでなく、うつや不安、痛みへの恐怖心といった心理的な側面にも大きな治療効果をもたらすことが示されています。
介入による改善効果は半年から2年以上にわたって持続し、従来の認知行動療法(CBT)に匹敵する成果を上げている点が特徴です。
一方で、プログラムが長期にわたるため、急性腰痛への適用や比較検証については依然として課題が残されていることも指摘されています。
総じて、薬物に頼らない統合的な治療アプローチとして、MBSRが現代の腰痛管理において極めて重要な役割を担っていることを包括的に解説しています。
目次
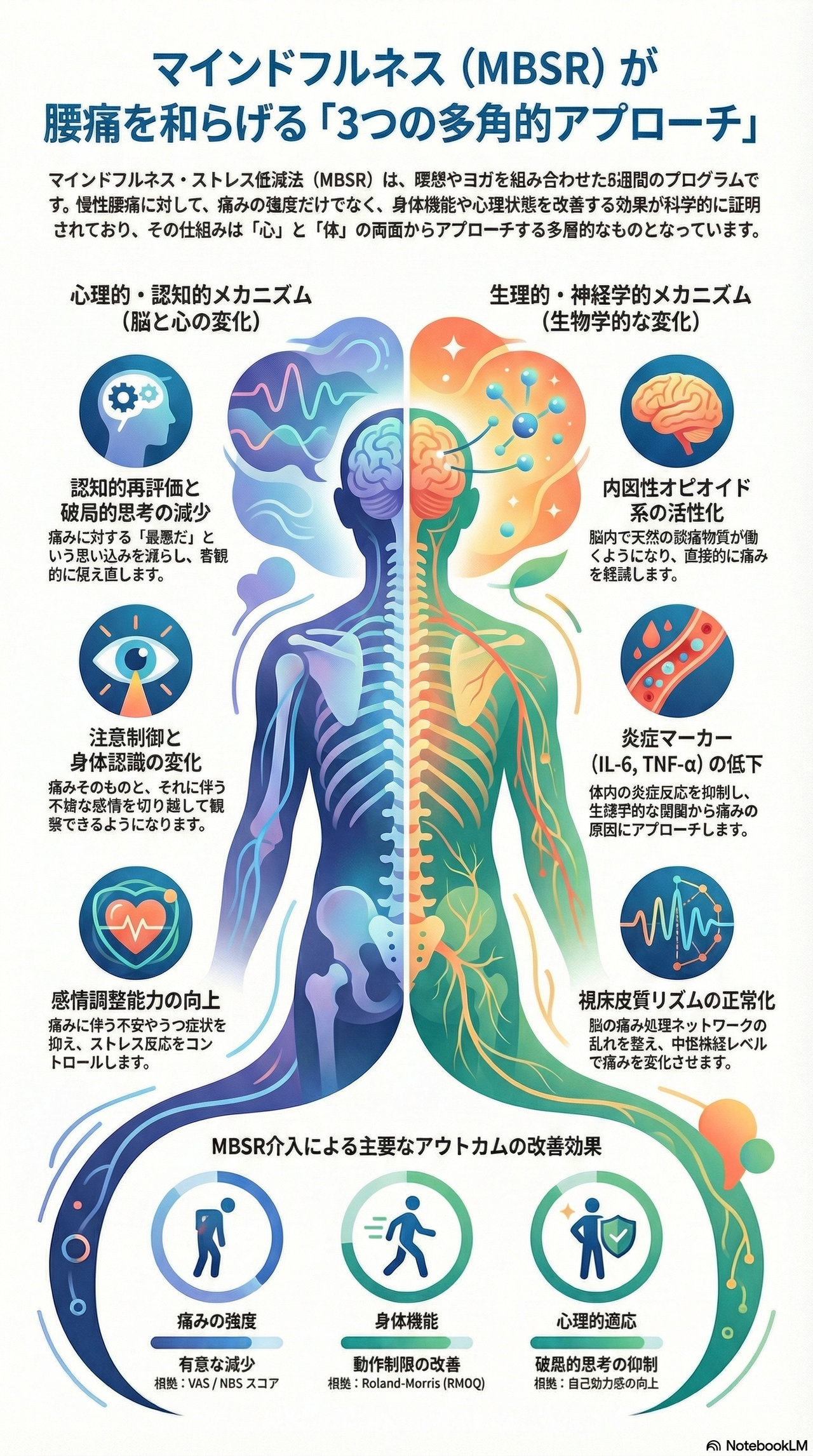
マインドフルネス・ストレス低減法(MBSR)が腰痛、特に慢性腰痛を和らげる具体的な仕組みは、単一の要因ではなく、心理的側面と神経生理学的(生物学的)側面の両面から構成されています。
参考文献に基づいた具体的なメカニズムは以下の通りです。
MBSRは、「今この瞬間に、意図的に、判断せずに注意を向ける」というマインドフルネスの概念を通じて、痛みに対する捉え方や反応を変化させます。
- 破局的思考の減少(認知的再評価): 痛みに対して「もう治らない」「耐えられない」といった過度に否定的な評価(破局的思考)を減らすことが、重要な作用機序の一つです。
- 注意制御の向上: 痛みという刺激に対して柔軟に注意を転換できるようになり、痛みに過度に集中し続ける状態を改善します。
- 感情調整と感覚の分離: 痛みを「身体的な感覚」と「それに伴う不快な感情(苦しみ)」に分離して捉えられるようになります。これにより、痛みに伴う否定的感情への対処能力が向上します。
- 自己効力感と自己慈悲の向上: 痛みに対処できるという自信(自己効力感)を高め、自分自身に対する優しさや理解(自己慈悲)を深めることで、心理的な適応を助けます。
- 恐怖回避信念の修正: 痛みに対する恐怖から活動を避けてしまう「恐怖回避信念」を修正し、機能改善を促します。
MBSRの効果は心理的な変化にとどまらず、身体の生物学的なプロセスにも直接影響を与えることが示唆されています。
- 内因性オピオイド系の活性化: マインドフルネス瞑想が、体内の自然な鎮痛物質である内因性オピオイド系を介して、痛みを直接的に軽減する可能性が報告されています。
- 炎症マーカーの低下: 炎症に関連する物質(IL-6、TNF-αなど)のレベルを低下させることが示されています。
- ストレス反応の抑制: 生理学的なストレス指標であるコルチゾールレベルの増加を抑制し、身体のストレス反応を穏やかにします。
- 視床皮質リズムの正常化: 慢性疼痛の神経生理学的な基盤の一つとされる「視床皮質ディスリズミア(thalamocortical dysrhythmia)」を改善し、中枢神経系レベルで痛みの処理を変化させる可能性が示されています。
内因性オピオイド系が活性化するとは、簡単に言うと**「身体が自ら作り出す天然の鎮痛物質(内因性オピオイド)が放出され、脳や神経系で痛みを抑える仕組みが働くこと」**を指します。
- 天然の鎮痛メカニズム: 内因性オピオイド系は、体内に備わっている自然な鎮痛システムです。マインドフルネス瞑想を行うことでこのシステムが活性化され、慢性腰痛を直接的に軽減する可能性が示されています。
- プラセボ(偽薬)効果ではない実体: この活性化は、単なる「思い込み」や心理的なプラセボ効果ではなく、具体的な神経生理学的メカニズムに基づいた反応であることが研究(Khatib et al., 2024)によって示唆されています。
- 脳レベルでの変化: 瞑想による内因性オピオイド系の活性化は、中枢神経系(脳や脊髄)のレベルで痛みの処理を変化させ、痛みの知覚そのものを和らげる役割を果たします。
- オピオイド処方患者への意義: MBSRはこの内因性オピオイド系に働きかけるため、すでに鎮痛剤としてオピオイドを使用している慢性腰痛患者においても、痛みの軽減や薬の減量を支援する有効な手段となり得ると考えられています。
つまり、内因性オピオイド系の活性化とは、マインドフルネスの実践を通じて**「脳が自ら痛み止めを分泌し、物理的に痛みを緩和する状態になること」**を意味しています,。
視床皮質リズムの正常化は、脳において主に**「慢性疼痛の神経生理学的な基盤を改善し、中枢神経系レベルでの痛み処理を変化させる」**という重要な影響を与えます。
- 脳内のリズムの乱れ(ディスリズミア)の修復: 慢性疼痛を抱える患者の脳では、視床(感覚を中継する部位)と大脳皮質の間でやり取りされる信号のリズムが乱れる「視床皮質ディスリズミア(thalamocortical dysrhythmia)」という状態が、痛みの原因の一つと考えられています。MBSRの実践はこの乱れたリズムを改善する可能性が示されています。
- 中枢神経系レベルでの処理の変化: このリズムが正常化されることは、脳が痛みの信号を処理する方法そのものが変化することを意味します。これにより、末梢からの刺激に対して脳が過剰に反応したり、痛みを増幅させたりするプロセスが抑えられます。
- 慢性疼痛の基盤へのアプローチ: 視床皮質リズムの正常化は、痛みの感覚を単に一時的に和らげるのではなく、「慢性疼痛を生み出している脳の仕組み」そのものに働きかける生物学的なメカニズムの一つとして位置づけられています。
このように、視床皮質リズムが正常化されることで、脳は痛みの信号をより適切に処理できるようになり、それが慢性腰痛の軽減へとつながると考えられています。
視床皮質ディスリズミアの改善とは、一言で言えば**「脳内の情報伝達における『リズムの乱れ』を整え、痛みを処理する仕組みを正常化すること」**を指します。
- 脳内のコミュニケーションの正常化: 視床皮質ディスリズミアとは、感覚を中継する「視床」と、それを処理する「大脳皮質」の間でやり取りされる神経信号のリズムが乱れている状態を指します。このリズムの乱れは、慢性疼痛を引き起こす神経生理学的な基盤の一つと考えられています。
- 中枢神経系レベルでの変化: MBSR(マインドフルネス・ストレス低減法)の実践によってこのディスリズミアが改善されることは、中枢神経系のレベルで痛みの処理方法そのものが変化することを意味します。つまり、脳が痛みの信号を過剰に増幅したり、誤って処理したりする状態が修正されるということです。
- 生物学的なメカニズムの裏付け: この改善は、MBSRの効果が単なる心理的なプラセボ(偽薬)効果ではなく、具体的な脳の生物学的メカニズムに基づいていることを示す重要な知見として報告されています。
視床皮質ディスリズミアの改善とは、マインドフルネスを通じて**「慢性的な痛みを発生させている脳のリズムの不具合」を物理的に調整し、痛みの感じ方そのものを根本から変えること**を意味しています。
マインドフルネス(特にMBSR)によって炎症マーカーが低下する理由は、マインドフルネスの実践が身体のストレス反応と炎症反応に直接的な影響を与えるためと考えられています。
- ストレス反応の抑制: MBSRの実践は、生理学的なストレス指標であるコルチゾールレベルの増加を抑制することが示されています。コルチゾールはストレス下で放出されるホルモンであり、これが増加すると身体の様々な機能に影響を与えますが、マインドフルネスはこの反応を穏やかにします。
- 炎症プロセスの直接的な改善: マインドフルネスは、体内の炎症に関わる具体的な物質である**IL-6(インターロイキン-6)やTNF-α(腫瘍壊死因子アルファ)**といった炎症マーカーのレベルを低下させることが研究で確認されています。
- 生物学的な相互作用: これらの変化は、マインドフルネスが単に心理的な変化をもたらすだけでなく、身体の生物学的なプロセス(炎症反応システム)に直接介入し、それを正常化する働きを持っていることを示唆しています。
慢性腰痛における**「中枢性感作(ちゅうすうせいかんさ)」**とは、痛みが長期間(通常3ヶ月以上)続くことで、中枢神経系(脳や脊髄)が痛みに対して過敏になり、本来なら痛みを感じないような刺激でも痛みとして捉えたり、わずかな痛みを増幅させて感じたりする状態を指します。
参考文献に基づく具体的な特徴と、MBSRとの関連については以下の通りです。
急性腰痛の主な原因は組織の損傷や炎症ですが、慢性腰痛ではこの「中枢性感作」が重要な役割を果たします。
- 急性腰痛: 主に身体的な組織損傷に関連し、心理社会的要因の関与は相対的に少ない。
- 慢性腰痛: 中枢性感作に加え、痛みの破局化(過度に否定的に考えること)、恐怖回避信念(痛みを恐れて動かなくなること)、うつや不安といった心理社会的要因が複雑に絡み合っています。
中枢性感作の具体的な現れの一つとして、ソースでは**「視床皮質ディスリズミア(thalamocortical dysrhythmia)」**が挙げられています。
- これは、脳内の感覚を中継する部位(視床)と処理する部位(大脳皮質)の間のコミュニケーション・リズムが乱れている状態です。
- このリズムの乱れが、中枢神経レベルで痛みを増幅させ、慢性疼痛を維持させる基盤となっていると考えられています。
中枢性感作を起こしている脳は、心理的なストレスや否定的な思考によってさらに痛みに敏感になります。MBSRは以下の経路でこの悪循環を断ち切ると考えられています。
- 認知的・心理的介入: 破局的思考や恐怖回避信念を修正することで、脳が痛みを「脅威」と見なす度合いを減らします。
- 生理的変化: 前述の「視床皮質リズム」を正常化させたり、内因性オピオイド系(天然の鎮痛システム)を活性化させたりすることで、中枢神経系における痛みの処理プロセスそのものを変化させます。
このように、慢性腰痛が単なる「腰の筋肉や骨の問題」ではなく、**「脳を含む神経系の過敏状態(中枢性感作)」**へと移行しているからこそ、思考や意識の向け方を変えるマインドフルネス(MBSR)が有効な治療選択肢となり得るのです。
マインドフルネス・ストレス低減法(MBSR)と認知行動療法(CBT)は、どちらも慢性腰痛に対して**「同等の臨床的効果」を示すことが複数の大規模な研究で確認されていますが、その「アプローチ(手法)」や「作用機序(仕組み)」**には違いがあります。
- 痛みの強度と機能制限の改善: 介入直後から26週、52週、さらには2年後の追跡調査においても、両者は痛みの軽減と身体機能の改善において同様の結果を維持しています。
- 心理的要因への影響: どちらの療法も、破局的思考(痛みを過度に否定的に考えること)の減少、うつ症状の改善、自己効力感の向上に寄与します。
- MBSR(マインドフルネス): 「今この瞬間に、判断せずに注意を向けること」を重視します。具体的には、ボディスキャン、座位瞑想、ヨガなどを通じて、「痛みの感覚」と「それに伴う感情的な反応」を分離して捉える訓練を行います。
- CBT(認知行動療法): 痛みに関連する否定的な思考パターンや行動を特定し、それをより適応的なものへと再構築することに焦点を当てます(認知的再構築や行動活性化など)。
- MBSR特有の可能性: マインドフルネスは、内因性オピオイド系(天然の鎮痛システム)の活性化や、視床皮質リズムの正常化といった、より直接的な神経生理学的変化を介して痛みを軽減する可能性が示唆されています。
- CBTの側面: メタ分析によると、CBTは通常ケアと比較して**「恐怖回避信念(痛みを恐れて動かなくなること)」の修正**に有意な差が認められたという報告がありますが、MBSRにおけるこの変化については明確な報告が不足している場合があります。
MBSRは、特に**「従来の治療に反応しない患者」や「心理社会的要因が顕著な患者」、「非薬物的なアプローチを好む患者」**にとって有力な選択肢となります。
一方で、マインドフルネスと認知療法の要素を統合した「マインドフルネス認知療法(MBCT)」の方が、瞑想単独よりも長期的な効果が大きい可能性も示唆されています。
**マインドフルネス認知療法(MBCT)**は、マインドフルネスの要素と認知療法の要素を統合した手法です。
参考文献に基づいた主な特徴と効果は以下の通りです。
MBCTは、マインドフルネス瞑想(MM)のトレーニングに、認知療法の特定の技法を組み合わせたアプローチです。参考文献では、**「マインドフルネスと認知療法の要素を統合することで、より持続的な効果が得られる可能性」**が示唆されています。
慢性腰痛患者を対象とした研究(Day et al., 2019)では、MBCTの効果について以下のような知見が報告されています。
- 身体機能と痛みの干渉: 介入直後の身体機能に大きな改善が見られるだけでなく、3ヶ月および6ヶ月の追跡調査において、マインドフルネス瞑想単独(MM)の参加者よりも、痛みの干渉や身体機能において有意に大きな改善を示しました。
- 心理的改善: 治療後のうつ病スコアも大幅に改善し、追跡調査でも瞑想単独群よりMBCT群の方が高い改善効果を維持していました。
これまでの回答で触れたMBSRはマインドフルネス瞑想を中心としたプログラムですが、MBCTはそこに**「認知療法(CBT)」の要素を明示的に組み込んでいる点**が特徴です。この統合によって、瞑想単独よりも長期的かつ持続的な効果が期待できると考えられています。
総じて、MBCTはマインドフルネスによる「今ここ」への気づきと、認知療法による「思考パターンの再構築」を掛け合わせることで、慢性腰痛に伴う身体的制限や心理的苦痛に対してより強力にアプローチする手法といえます。
標準的なマインドフルネス・ストレス低減法(MBSR)は、ジョン・カバット・ジンによって開発された8週間の構造化されたプログラムであり、主に以下の練習や要素で構成されています。
- グループセッション: 週に1回、約2〜2.5時間のセッションを8週間行います。
- 集中リトリート: プログラムの期間中に、1日(通常6〜7.5時間)の集中セッションが行われます。
- 自宅練習: 毎日約45分間の自主練習が推奨されています。
- ボディスキャン: 身体の隅々に意識を向け、その時々の感覚を判断せずに観察する練習です。
- 座位瞑想(ざいめいそう): 静かに座り、呼吸や身体の感覚、湧き上がる思考や感情に注意を向ける練習です。
- ヨガ: ゆっくりとした動きの中で身体の感覚に意識を向ける、マインドフル・ヨガが含まれます。
- 歩行瞑想: 歩くという動作に伴う足の裏の感覚などに注意を向ける練習です。
- 日常生活への統合: 食べる、掃除をする、対話をするなど、日常のあらゆる活動の中にマインドフルネス(今この瞬間に、判断せずに注意を向けること)を取り入れる練習です。
[1] Serrat, M., Almirall, M., Musté, M., Sanabria-Mazo, J. P., Feliu-Soler, A., Méndez-Ulrich, J. L., Luciano, J. V., & Sanz, A. (2021). Effectiveness of a Multicomponent Treatment based on Pain Neuroscience Education, Therapeutic Exercise, Cognitive Behavioural Therapy, and Mindfulness in Patients with Fibromyalgia (FIBROWALK study): A Randomized Controlled Trial. Physical Therapy. https://doi.org/10.31234/OSF.IO/KJ8SP
[2] Eiger, C., Keogh, A., Rogan, S., & Swanenburg, J. (2025). Pain Science Education for Patients with Chronic Pain Referred to Community-Based Rehabilitation: Translation, Adaptation, and Clinical Feasibility Testing of PNE4Adults. Stomatology. https://doi.org/10.3390/jcm14030771
[3] Moseley, G. L., Gallace, A., & Spence, C. (2023). Teaching patients about pain: the emergence of Pain Science Education, its learning frameworks and delivery strategies. The Journal of Pain. https://doi.org/10.1016/j.jpain.2023.11.008
[4] Miller, C. A., Williams, M. M., Holtgrieve, M. M., & Ciol, M. A. (2017). Depicting individual responses to physical therapist led chronic pain self-management support with pain science education and exercise in primary health care: multiple case studies. https://doi.org/10.1186/S40945-017-0032-X
[5] Johnson, A. P., Simonson, D. C., Guck, T. P., Meilman, S. E., & Dompier, T. P. (2025). The Effects of Physical Therapy Management and Pain Neuroscience Education on Patients With Musculoskeletal Pain Undergoing Rehabilitation for Substance Use Disorder: A Quality Improvement Project. JOSPT open. https://doi.org/10.2519/josptopen.2025.0111
[6] Galan-Martin, M. A., Montero-Cuadrado, F., Lluch-Girbes, E., Coca-López, M. C., Mayo-Iscar, A., & Cuesta-Vargas, A. (2020). Pain Neuroscience Education and Physical Therapeutic Exercise for Patients with Chronic Spinal Pain in Spanish Physiotherapy Primary Care: A Pragmatic Randomized Controlled Trial. Journal of Clinical Medicine. https://doi.org/10.3390/JCM9041201
[7] Louw, A., Zimney, K., Puentedura, E. J., & Diener, I. (2017). A clinical perspective on a pain neuroscience education approach to manual therapy. Journal of Manual & Manipulative Therapy. https://doi.org/10.1080/10669817.2017.1323699
[8] Schneider, C. (2025). Patient:innen profitieren von Informationen. Deleted Journal. https://doi.org/10.1007/s00132-025-04702-y
[9] Salazar‐Méndez, J., Cuyul-Vásquez, I., Méndez-Rebolledo, G., Gutiérrez-Espinoza, H., Sánchez-Romero, E. A., Araya-Quintanilla, F., & Fernández-Carnero, J. (2024). Effectiveness of in-group versus individually administered pain neuroscience education on clinical and psychosocial outcomes in patients with chronic low back pain: randomized controlled study protocol. PeerJ. https://doi.org/10.7717/peerj.17507
[10] Nijs, J., Paul van Wilgen, C., Van Oosterwijck, J., van Ittersum, M., & Meeus, M. (2011). How to explain central sensitization to patients with 'unexplained' chronic musculoskeletal pain: Practice guidelines. Manual Therapy. https://doi.org/10.1016/J.MATH.2011.04.005
[11] Lima, M. de O., Guimarães, A. T. B., Resende, M. A., & Caramelli, B. (2021). Educação em dor em pacientes com lombalgia e sensibilização central: um estudo piloto. Research, Society and Development. https://doi.org/10.33448/RSD-V10I11.19715
[12] Nijs, J., Malfliet, A., Roose, E., Labie, C., Rheel, E., Leysen, L., Wilgen, C. P. van, & Dankaerts, W. (2020). Integrating motivational interviewing in pain neuroscience education for people with chronic pain: a practical guide for clinicians. Physical Therapy. https://doi.org/10.1093/PTJ/PZAA021
[13] Alsamti, A. M., Alsamti, A. M., Alsamti, A. M., Alsamti, A. M., Alsamti, A. M., Alsamti, A. M., Alsamti, A. M., Alsamti, A. M., Alsamti, A. M., & Alsamti, A. M. (2025). Management of Chronic Pain in Family Medicine Roles of Nursing, Anesthesia, Medical Coding, Radiology, and Intensive Care. International journal of computational and experimental science and engineering. https://doi.org/10.22399/ijcesen.3975
[14] Nijs, J., Roussel, N., Paul van Wilgen, C., Köke, A., & Smeets, R. (2010). Primary Care Physical Therapy in People With Fibromyalgia: Opportunities and Boundaries Within a Monodisciplinary Setting. Physical Therapy. https://doi.org/10.2522/PTJ.20100046
[15] Malfliet, A., Kregel, J., Coppieters, I., De Pauw, R., Meeus, M., Roussel, N., Cagnie, B., Danneels, L., & Nijs, J. (2018). Effect of pain neuroscience education combined with cognition-targeted motor control training on chronic spinal pain: a randomized clinical trial. JAMA Neurology. https://doi.org/10.1001/JAMANEUROL.2018.0492
[16] Sutton, K. Pain neuroscience education as an intervention for chronic pain.
[17] Cuenca-Martínez, F., Suso-Martí, L., Varangot-Reille, C., Herranz-Gómez, A., Blanco-Díaz, M., & Sanz-Corbalán, I. (2022). Effectiveness of pain neuroscience education (pne) in patients with persistent pain due to fibromyalgia. EDULEARN proceedings. https://doi.org/10.21125/edulearn.2022.1050
[18] Minen, M. T., Jalloh, A., Begasse de Dhaem, O., & Seng, E. K. (2021). Neuroscience education as therapy for migraine and overlapping pain conditions: a scoping review. Pain Medicine. https://doi.org/10.1093/PM/PNAB131
[19] Alagappan, U., Mani, R., Sharma, S., & Acharya, R. Effect of Biopsychosocial Comprehensive Chronic Pain Management Physiotherapy Practice Protocol in Patients with Chronic Musculoskeletal Pain-a Randomised Control Trial. https://doi.org/10.18203/2349-3259.ijct20250133
[20] Nijs, J., Paul van Wilgen, C., Van Oosterwijck, J., van Ittersum, M., & Meeus, M. How to explain central sensitization to patients with 'unexplained'chronic musculoskeletal pain: practice guidelines.
[24] Fernández-Gualda, E., Obrero-Gaitán, E., Rodríguez-Almagro, D., Osuna-Pérez, M. C., Cortés-Pérez, I., Ibancos-Losada, M. del R., & López-Ruiz, M. del C. (2023). Persistent pain management in an oncology population through pain neuroscience education, a multimodal program: PaiNEd randomized clinical trial protocol. PLOS ONE. https://doi.org/10.1371/journal.pone.0290096
[26] Wenger, N., Sheth, M., Sansone, C., Stuck, A., Hreha, K., & Haas, M. (2018). Reducing Opioid Use for Patients With Chronic Pain: An Evidence-Based Perspective. Physical Therapy. https://doi.org/10.1093/PTJ/PZY025
[27] Diener, I. (2021). Physiotherapy support for self-management of persisting musculoskeletal pain disorders. South African journal of physiotherapy. https://doi.org/10.4102/SAJP.V77I1.1564
[29] Kjaer, P., Kongsted, A., Ris, I., Abbott, A., Rasmussen, C. D. N., Roos, E. M., Skou, S. T., Andersen, T. E., & Hartvigsen, J. (2018). GLA:D ® Back group-based patient education integrated with exercises to support self-management of back pain - development, theories and scientific evidence. BMC Musculoskeletal Disorders. https://doi.org/10.1186/S12891-018-2334-X
[30] Manfuku, M., Nishigami, T., Mibu, A., Yamashita, Y., Imai, R., Tanaka, K., Kitagaki, K., Deie, M., & Matsuo, T. (2021). Effect of perioperative pain neuroscience education in patients with post-mastectomy persistent pain: a retrospective, propensity score-matched study. Supportive Care in Cancer. https://doi.org/10.1007/S00520-021-06103-1
ごあいさつ

長引いた痛みを一人で治すのは困難なことが多いです。
困ったときは自身で判断せずに適切な処置を受けるために専門家に相談しましょう。
もし、お近くにお住まいで、困っているならば、一度ひまわり接骨院までお問い合わせください。腰痛・坐骨神経痛の専門家の新幡が、ご相談に乗ります。
気軽にご相談ください。

新着情報・お知らせ
お気軽にお問合せください

お電話でのお問合せ・相談予約
<受付時間>
月~土
9:00〜13:00 /15:00〜19:00
※日曜・祝日は除く
フォームは24時間受付中です。お気軽にご連絡ください。
ひまわり接骨院

住所
〒213-0002
神奈川県川崎市高津区二子1丁目7−17 リバーサイドマンション杉崎 102
アクセス
二子新地駅 徒歩3分
駐車場:近隣にコインパーキングあり。自転車・バイクは店舗前に駐輪場がございます。
受付時間
月~土
9:00〜13:00 /15:00〜19:00
定休日
日曜・祝日

