
〒213-0002 神奈川県川崎市高津区二子1丁目7−17
リバーサイドマンション杉崎 102 二子新地駅 徒歩3分
| 月 | 火 | 水 | 木 | 金 | 土 | 日祝 | |
|---|---|---|---|---|---|---|---|
| 9:00〜13:00 | ● | ● | ● | ● | ● | ● | ─ |
| 15:00〜19:00 | ● | ● | ● | ● | ● | ● | ─ |
腰椎すべり症の運動療法:エビデンスに基づく包括的ガイド
公開日:2026/04/30
更新日:2026/06/29
このページでは、腰椎すべり症に対して手術を行わずに改善を目指す運動療法の有効性について、国内外のガイドラインや科学的根拠を基に解説しています。
主な内容として、体幹の安定化や柔軟性の向上、神経への圧迫を和らげるための具体的な運動法が詳しく紹介されています。
特に軽度から中等度の症状を持つ患者には、まず3〜6ヶ月間の保存療法を優先することが推奨されており、早期の手術回避が可能である点も強調されています。
また、治療の成功には患者ごとの個別プログラムと、教育を通じた長期的な自己管理が不可欠であると結論づけています。
最終的に、運動療法は単なる一時しのぎではなく、痛みの根本解決と生活の質の向上を目指すための積極的な治療手段として位置づけられています。
目次
参考文献に基づいて、腰椎すべり症に対する運動療法の概要をまとめます。
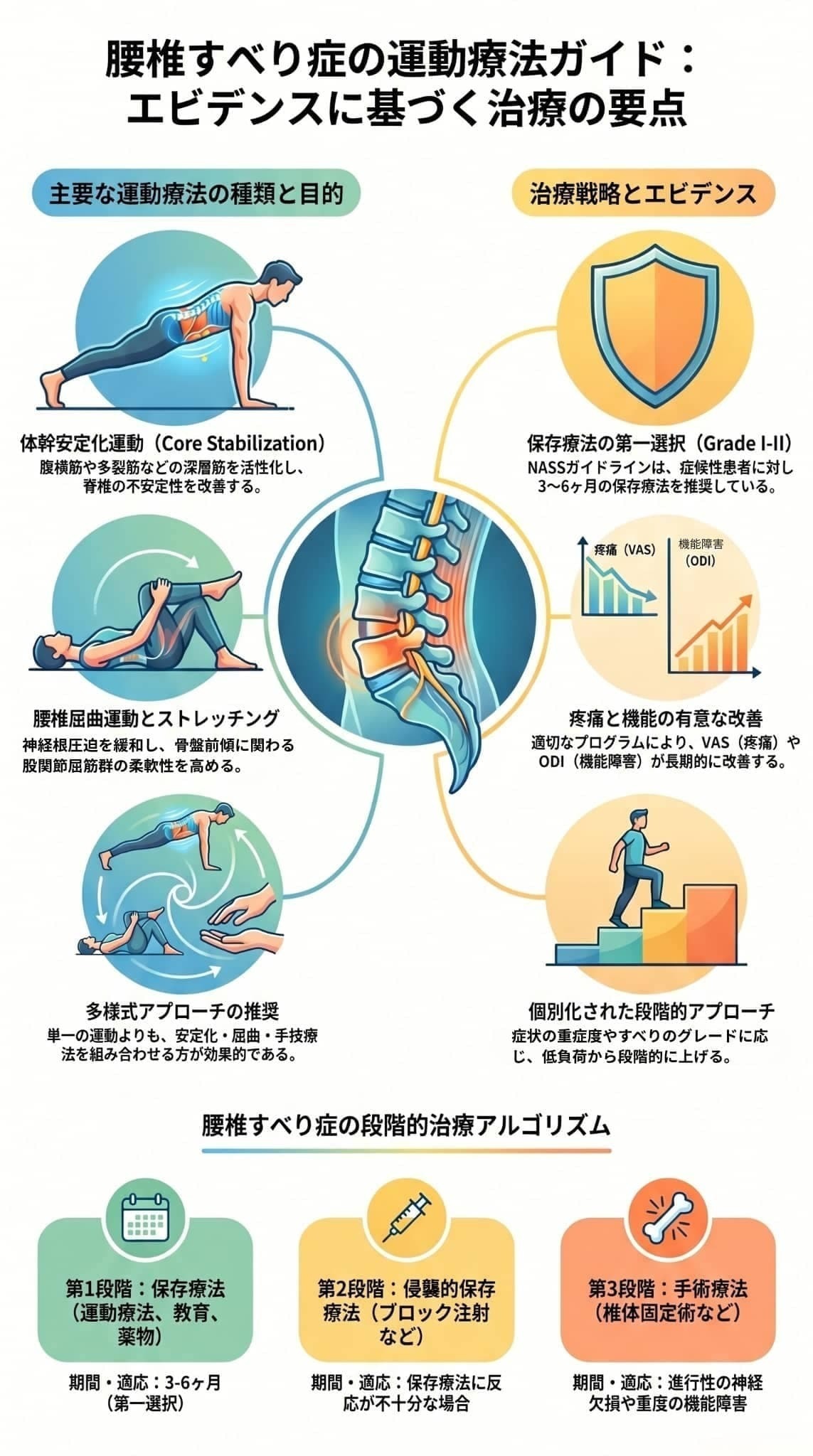
腰椎すべり症に対する運動療法は、特に低グレード(Grade I-II)の患者において、痛みの軽減、機能障害の改善、生活の質(QOL)の向上に有効であることが示されています。
北米脊椎外科学会(NASS)をはじめとする多くのガイドラインでも、まずは運動療法などの保存療法を試みることが推奨されています。
- 目的: 腹横筋、多裂筋、骨盤底筋、横隔膜といった「深層体幹筋」を選択的に活性化させ、脊椎の不安定性を改善します。
- 具体的な運動: 腹横筋を収縮させるドローイン、仰向けでの骨盤挙上(ブリッジング)、プランク、四つ這いでの対角線運動などがあります。
- 目的: 腰椎を反る(伸展する)ストレスを軽減し、椎間孔(神経の通り道)を広げることで、神経根への圧迫を和らげます。
- 具体的な運動: 膝を胸に近づける運動(膝胸運動)、骨盤の後傾運動、猫背運動(Cat-camel exercises)などがあります。
- 目的: 腰椎のバイオメカニクス(生体力学)を正常化するために、筋肉の短縮や拘縮を改善します。
- 対象となる主な筋肉: 腸腰筋などの股関節屈筋群、太もも裏のハムストリングス、お尻の梨状筋、腰背筋群などが推奨されます。
- マニュアルセラピー: 関節モビライゼーションやマニピュレーションなどの徒手療法が用いられることもありますが、すべりの程度が強い(高グレード)場合や、神経学的な症状がある場合は禁忌とされることが多いです。
- 有酸素運動: 全身の体力向上や体重管理のために、歩行、水中運動、固定式自転車といった体への衝撃が少ない運動が推奨されます。
- 胸椎モビライゼーション: 胸椎(背中)の動きを良くすることで、腰への代償的な負担を減らします。
- 多様式介入: 単一の運動だけでなく、体幹安定化運動、ストレッチング、有酸素運動、患者教育などを組み合わせた包括的なプログラムが推奨されます。
- 段階的プログレッション: 初めは低負荷・低難易度のものから開始し、患者の耐性や進歩に合わせて徐々に負荷を上げていくことが重要です。
- 個別化されたアプローチ: すべての患者に同じ運動が適しているわけではなく、年齢、すべりのタイプやグレード、症状の重さ、患者の希望などに合わせた個別の治療計画が必要です。
ただし、現状のエビデンスには「研究規模が小さい」「運動のメニューや頻度が研究によってバラバラである」「長期的なデータが不足している」といった限界があり、どの運動療法が最も効果的かという明確なコンセンサスはまだ得られていない点には留意が必要です。
腰椎すべり症に対する具体的な運動の種類と方法について、以下に詳しく解説します。
- ドローイン(Abdominal drawing-in): お腹をへこませるようにして、腹横筋を選択的に収縮させる運動です。
- ブリッジング(Bridging): 仰向け(仰臥位)に寝た状態で、骨盤を上に持ち上げる運動です。
- プランク(Plank): うつ伏せ(腹臥位)の状態から前腕とつま先で体を支え、体幹を真っ直ぐに保持する運動です。
- 四つ這い位での対角線運動(Quadruped diagonal exercises): 四つ這いの状態から対角線上にある手と足を同時に伸ばすなどして、バランスと協調性を向上させる運動です。
- 膝胸運動(Knee-to-chest exercises): 仰向けの状態で膝を曲げ、両手で抱え込んで胸に近づける運動です。
- 骨盤後傾運動(Pelvic tilt exercises): 骨盤を後ろに傾ける運動です。
- ウィリアムズ屈曲運動(Williams flexion exercises): 腰椎を屈曲させることを目的とした一連の運動プログラムです。
- 猫背運動(Cat-camel exercises): 四つ這いの状態で、背中を丸めたり反らしたりする運動です。
- 股関節屈筋群: 腸腰筋、大腿直筋など(股関節の前側の筋肉)。
- ハムストリングス: 太ももの裏側の筋肉。
- 梨状筋: お尻の奥にある筋肉。
- 腰背筋群: 腰から背中にかけての筋肉。
- 有酸素運動: 全身的な体力向上、体重管理、心理的健康の改善のために、歩行、水中運動、固定式自転車など、体への衝撃が少ない(低衝撃)運動が推奨されます。
- McKenzie(マッケンジー)法: 特定の方向性を持たせた反復運動を用いて、痛みを軽減・局所化(中心化)させることを目指すアプローチです。
- 胸椎モビライゼーション: 胸椎(背中部分の背骨)の動きが制限されると腰椎に代償的な負担がかかるため、胸椎の動きを改善するアプローチも推奨されています。
- マニュアルセラピー: 関節のモビライゼーションやマニピュレーションといった徒手療法が行われることもありますが、すべり症の程度が強い(高グレード)場合や神経学的な症状を伴う場合は禁忌とされることが多いため、実施には慎重な判断が必要です。
腰椎すべり症に対する運動療法は、特に低グレード(Grade I-II)の患者において、疼痛の軽減、機能障害の改善、生活の質の向上に有効であることが、複数のシステマティックレビューやランダム化比較試験(RCT)によって示されています。
- 長期的な痛みの軽減: O'Sullivanらの先駆的研究(1997年)では、腹横筋や多裂筋をターゲットにした特異的安定化運動を10週間行った結果、Visual Analogue Scale(VAS)による疼痛スコアとOswestry Disability Index(ODI)による機能障害スコアが有意に改善しました。注目すべき点として、この効果は30ヶ月後の追跡調査でも維持されていました。
- 短期的な痛みの軽減: Nava-Bringasらの研究(2014年)においても、8週間の安定化運動プログラムにより、機能性の改善とともに疼痛の有意な減少が確認されています。
- 歩行能力などの機能向上: Jainらの研究(2022年)では、多様式理学療法リハビリテーションを実施した後、患者の立位時間および歩行時間が延長したことが報告されています。また、Kaurらの研究(2023年)では、体幹強化運動によって腰椎の可動域が改善したとされています。
運動療法の有効性は国際的なガイドラインでも支持されています。
- 北米脊椎外科学会(NASS)のガイドライン: 症候性の変性すべり症患者に対して、まずは運動療法などの保存療法を試みることが推奨されています。
- 適切使用基準(AUC): Reitmanら(2021年)が開発した基準において、特に軽度から中等度の症状を有する患者に対する理学療法(運動療法を含む)の適切性が確立されています。
手術療法(椎体固定術)と保存療法を比較した場合、短期的には手術の方が疼痛や機能障害の改善において優れる可能性があるものの、長期的な転帰における明確な優位性は確立されていません。多くの患者が保存療法のみで症状の改善を得られるため、まずは段階的な治療アプローチとして運動療法を行うことが強く推奨されています。
これらの有効性が示されている一方で、現在存在するエビデンスにはいくつかの重要な限界が指摘されており、「どの運動療法が最も効果的か」という明確なコンセンサスにはまだ至っていません。
- 研究の規模と質の限界: 多くの研究はサンプルサイズが小さく(小規模)、統計的な検出力が不足しています。また、適切な対照群(プラセボなど)を設定した研究が少ないことも指摘されています。
- 介入内容のバラつき(異質性): 運動の種類、頻度、期間といったプロトコルが研究によって大きく異なるため、エビデンスを画一的に評価することが困難です。
- データ不足: 疼痛や機能障害の改善がQOLの向上につながることは示唆されているものの、QOLを主要な評価基準とした大規模研究や、長期的な効果・再発率を追跡したデータが不足しています。
これらの限界があるため、実際の臨床では、エビデンスに基づきながらも、患者個人の症状の重さ、すべりのグレード、機能的な要求(スポーツへの復帰など)に合わせた個別化された運動療法プログラムを提供することが不可欠とされています。
国際的なガイドラインにおける腰椎すべり症に対する推奨事項は、主に以下のようになっています。
多くのガイドラインにおいて、特に低グレード(Grade I-II)の腰椎すべり症患者に対しては、手術を検討する前にまず保存療法を試みることが共通して推奨されています。
- 症候性の患者に対しては、理学療法、運動療法、薬物療法、装具療法を含む保存療法を最初に試みることが推奨されます。
- ただし、どのような運動が効果的かといった詳細な運動プロトコルや、具体的な実施方法に関する記述は限定的です。
- ブラジルおよびチェコのガイドライン: 主に手術適応に焦点を当てつつも、保存療法と手術療法の適応や保存療法の役割について言及しています。
- アスリートに対する推奨: 若年アスリートに多く見られる峡部性すべり症において、保存療法を行うことの重要性が強調されています。
Reitmanら(2021年)が開発した変性すべり症管理のための適切使用基準(AUC)では、患者の症状の重さや画像所見などを考慮した結果、特に軽度から中等度の症状を持つ患者に対する理学療法(運動療法を含む)の適切性が確立されています。
国際的に「まずは保存療法から」という方針は一致していますが、運動療法の具体的な内容(どの運動を行うべきか)、期間、頻度などについては、現在あるエビデンスの質に限界があるため、強い推奨グレードを付与することが困難な状況にあります。
そのため、実際の臨床現場では、ガイドラインを参考にしつつも、患者個人の症状の重さやすべりのグレード、機能的な希望を考慮した個別化されたアプローチが重要視されています。
腰椎すべり症に対する運動療法の安全性と禁忌に関する主な留意点は以下の通りです。
- 高グレードのすべり症や神経症状がある場合のマニピュレーション: 関節モビライゼーションやマニピュレーションなどのマニュアルセラピー(徒手療法)を取り入れる際は慎重な適応判断が求められ、特に高グレードのすべり症や神経学的な症状を伴う症例においては禁忌とされることが多いです。
- 進行性の神経症状などがある場合: 運動療法などの保存療法に反応しない持続的な痛みがある場合や、進行性の神経学的欠損(神経の圧迫による麻痺などの進行)、重度の機能障害がみられる場合は手術療法の適応となるため、無理に運動療法を継続することは推奨されません。
- 段階的なプログレッション(負荷の調整): 運動療法を安全に進めるためには、低負荷・低難易度の運動から開始し、患者の耐性や進歩に応じて段階的に負荷や難易度を上げていくことが重要です。
- 腰椎の「反り(伸展)」ストレスの回避: 股関節の筋肉などが硬くなって短縮すると、骨盤の前傾が強まり、腰の反り(腰椎の前弯)が増加してすべりを悪化させる危険性があります。そのため、腰椎の伸展ストレスを軽減させる「腰椎屈曲運動」の実施や、正しい運動フォームを身につけるための患者教育が安全な治療に不可欠です。
- 低グレード患者が主な対象: 現在のガイドラインや研究において、運動療法を含めた包括的なプログラムが安全かつ有効と示されているのは、主に低グレード(Grade I-II)のすべり症患者です。
運動療法は全般的に安全性の高い保存療法ですが、患者の年齢、すべりのタイプやグレード、症状の重さなどを総合的に考慮した「個別化されたアプローチ」のもとで実施することが求められます。
腰椎すべり症の治療において、運動療法を含めた保存療法は**「最も初期に試みるべき第一選択(ファーストライン)の治療」**として位置づけられています。
一般的な治療アルゴリズムにおいて、運動療法は最初に選択される治療の土台となります。
- 第1段階(最初の3〜6ヶ月):運動療法、マニュアルセラピーなどの理学療法をはじめ、患者教育、薬物療法、必要に応じた装具療法などの保存療法をまず行います。
- 第2段階: 保存療法を行っても改善が不十分な場合に、神経根ブロックや硬膜外ステロイド注射などの侵襲的なアプローチが検討されます。
- 第3段階: これらの保存療法に反応せず痛みが持続する場合や、進行性の神経症状(麻痺など)、重度の機能障害がある場合、あるいは患者の強い希望がある場合に初めて「手術療法」が検討されます。
手術療法(椎体固定術など)と保存療法を比較すると、短期的には手術の方が痛みや機能障害の改善において優れている可能性が示唆されています。
しかし、長期的な経過を見た場合、手術療法が保存療法よりも明確に優れているというエビデンスは確立されていません。多くの患者が保存療法のみで症状の改善を得られるため、まずは運動療法などの保存療法から始めることが推奨されています。
- ガイドラインの推奨: 北米脊椎外科学会(NASS)をはじめとする国際的なガイドラインでも、症状のある患者に対して手術の前にまず保存療法を試みることが推奨されています。
- 適切使用基準(AUC): 患者の症状や画像所見に基づく基準においても、特に「軽度から中等度の症状」を持つ患者に対する理学療法(運動療法を含む)を行うことの適切性が確立されています。
主に**低グレード(Grade I-II)**の腰椎すべり症患者において、痛みや機能の改善、生活の質(QOL)向上に向けた中核的な治療として位置づけられています。
腰椎すべり症の治療において、手術を検討する前にまず3〜6ヶ月間の保存療法を継続することが一般的な治療アルゴリズムとして推奨されています。
- 3〜6ヶ月の保存療法に反応せず、痛みが持続している場合
- 進行性の神経学的欠損(神経症状や麻痺などが進行している状態)がみられる場合
- 日常生活に支障をきたす重度の機能障害がある場合
- 患者自身が手術を強く希望する場合
なお、手術の要否を判断するにあたっては、この保存療法の期間と効果(反応性)だけでなく、症状の重症度、すべりのグレード、脊柱管狭窄の程度、患者の年齢や併存疾患なども総合的に考慮して決定されます。進行性の神経症状などがない限り、まずはこの3〜6ヶ月の期間を目安に保存療法に取り組むことで、多くの患者が手術を回避できる可能性があるとされています。
腰椎すべり症に対する運動療法の長期的な効果については、特定のプログラムで長期間の維持が確認されている一方で、全体としてはデータが不足しているというのが現状です。
腰椎すべり症の運動療法に関する包括的調査レポートの結論として、以下の重要なポイントが示されています。
具体的には、体幹安定化運動、腰椎屈曲運動、ストレッチング、マニュアルセラピーを含む包括的な運動療法プログラムが推奨されています。また、北米脊椎外科学会(NASS)のガイドラインでも、症状のある変性すべり症患者に対しては、まず保存療法を試みることが推奨されています。
手術療法と比べた場合、短期的には手術が優れる可能性があるものの、長期的には手術の明確な優位性は確立されていません。多くの患者が保存療法で改善を得られるため、まずは保存療法から始める段階的なアプローチが推奨されます。実際の臨床では、患者の症状の重さ、すべりのグレード、神経学的所見、機能面の希望などを考慮した個別化されたアプローチが不可欠です。治療を成功させるための鍵として、以下の要素が挙げられています。
- 体幹安定化運動を中心とした多様式介入
- 段階的な負荷の調整(プログレッション)
- 患者教育
- 長期的な自己管理の支援
運動療法の有効性が示される一方で、現在のエビデンスには「研究が小規模であること」「介入内容が研究間でバラバラであること」「長期的なアウトカムデータが不足していること」といった限界が存在します。
そのため、どの運動療法が最も効果的であるかについての明確なコンセンサスはまだ得られていません。これを克服するため、今後は標準化された介入プロトコルを用いた大規模なランダム化比較試験(RCT)や、長期フォローアップ研究、予後予測因子の同定、費用対効果の分析などが必要であると結論づけられています。
[1] Watters, W. C., et al. (2009). An evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spondylolisthesis. The Spine Journal, 9(7), 609-614. https://doi.org/10.1016/J.SPINEE.2009.03.016
[2] Matz, P. G., et al. (2016). Guideline summary review: an evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spondylolisthesis. The Spine Journal, 16(3), 439-448. https://doi.org/10.1016/J.SPINEE.2015.11.055
[3] Reitman, C. A., et al. (2021). Management of degenerative spondylolisthesis: development of appropriate use criteria. The Spine Journal, 21(7), 1256-1264. https://doi.org/10.1016/J.SPINEE.2021.03.005
[4] Baumann, A. N., et al. The impact of physical therapy interventions on pain and disability alleviation in adults with low grade lumbar spondylolisthesis: a systematic review of randomized controlled trials.
[5] Hasan, M., et al. (2023). Rehabilitation Protocol for spondylolisthesis Patients: A Treatment Protocol. Journal of Spine Research and Surgery, 5(1), 001-008. https://doi.org/10.26502/fjsrs0055
[6] Lawrance, M., et al. (2022). CURRENT CLINICAL CONCEPTS: Management of Common Lumbar Spine Posterior Column Disorders. Journal of Athletic Training, 57(11-12), 1030-1044. https://doi.org/10.4085/1062-6050-0161.21
[7] Zhang, Y., et al. (2025). [A prospective controlled study on degenerative lumbar spondylolisthesis treated with three steps and nine methods combined with physiotherapy]. Zhongguo Gu Shang, 38(1), 23-28. https://doi.org/10.12200/j.issn.1003-0034.20240592
[8] Briceño-González, M., et al. (2016). Guidelines for treatment of degenerative lumbar spondylolisthesis. Coluna/Columna, 15(3), 238-242. https://doi.org/10.1590/S1808-185120161503164082
[9] Rhajib, M. A., et al. Evidence based Physiotherapy Intervention of Lumbar Spondylolisthesis: A Narrative Review.
[10] Salsabil, N. Effectiveness of the McKenzie Treatment Protocol booklet for the patients suffering with Lumbar Spondylolisthesis: A Randomized Clinical Trial.
[11] Mironov, S. P., et al. (2020). Lumbosacral pain in athletes and ballet dancers: spondylolysis and spondylolisthesis. Conservative treatment. Traumatology and Orthopedics of Russia, 27(1), 11-18. https://doi.org/10.17816/VTO202027111-18
[12] Kaiser, R., et al. (2023). [Surgical Treatment of Degenerative Lumbar Stenosis and Spondylolisthesis: Clinical Practice Guideline]. Acta Chirurgiae Orthopaedicae Et Traumatologiae Cechoslovaca, 90(1), 21-30. https://doi.org/10.55095/achot2023/021
[13] Brearley, S., et al. (2021). Inter-Disciplinary Conservative Management of Bilateral Non-United Lumbar Pars Defects in a Junior Elite Golfer. The International Journal of Sports Physical Therapy, 16(1), 281-292. https://doi.org/10.26603/001C.18873
[14] Jain, S., et al. (2022). Changes in standing and walking time after multimodal physical rehabilitation in low grade degenerative lumbar spondylolisthesis: a non-randomised pilot study. Physiotherapy Theory and Practice, 38(13), 2867-2876. https://doi.org/10.1080/09593985.2022.2025965
[15] O'Sullivan, P. B., et al. (1997). Evaluation of Specific Stabilizing Exercise in the Treatment of Chronic Low Back Pain With Radiologic Diagnosis of Spondylolysis or Spondylolisthesis. Spine, 22(24), 2959-2967. https://doi.org/10.1097/00007632-199712150-00020
[16] Vanti, C., et al. (2021). Lumbar spondylolisthesis: STATE of the art on assessment and conservative treatment. Archives of Physiotherapy, 11(1), 19. https://doi.org/10.1186/S40945-021-00113-2
[17] Trăistaru, M. R., et al. (2022). Quality of life in osteoporotic patients with low-grade degenerative spondylolisthesis. Signa Vitae, 18(5), 86-92. https://doi.org/10.22514/sv.2022.022
[18] Nava-Bringas, T. I., et al. (2014). Effects of a stabilization exercise program in functionality and pain in patients with degenerative spondylolisthesis. Journal of Back and Musculoskeletal Rehabilitation, 27(1), 41-46. https://doi.org/10.3233/BMR-130417
[19] Luke, A., & Micheli, L. J. (2000). Spondylolysis and spondylolisthesis: principles in diagnosis and management. International Sportmed Journal, 1(4), 1-9.
[20] Reyes, A., & Rincón, E. (2014). La rehabilitación en la espondilólisis y la espondilolistesis. Revista Mexicana de Medicina Física y Rehabilitación, 26(2), 50-56.
[21] Kaur, M., et al. (2023). Efficacy of Core Strengthening Exercises and Interferential Therapy on Lumbar Range of Motion in Patients with Spondylolisthesis. International Journal of Health Sciences and Research, 13(12), 204-210. https://doi.org/10.52403/ijhsr.20231227
[22] Long, X., et al. Isthmic Spondylolisthesis: Interpretation of NASS Guidelines for Evidence-Based Medicine. https://doi.org/10.13210/j.cnki.jhmu.20190301.001
[23] Patel, D. R., et al. (2017). Evaluation and management of lower back pain in young athletes. Translational Pediatrics, 6(3), 225-235. https://doi.org/10.21037/TP.2017.06.01
[24] Rao, P. J., et al. (2023). A systematic review and meta-analysis with radiological correlation on the efficacy of spine stabilizing exercises in chronic low backache. International Journal of Orthopaedics Sciences, 9(4), 01-06. https://doi.org/10.22271/ortho.2023.v9.i4a.3466
[25] Theobald, C., et al. (2023). Non-operative treatment of degenerative spondylolisthesis. Seminars in Spine Surgery, 35(4), 101043. https://doi.org/10.1016/j.semss.2023.101043
[26] García, A. N., et al. (2015). Clinical approach to chronic lumbar pain: a systematic review of recommendations included in existing practice guidelines. Anales Del Sistema Sanitario De Navarra, 38(1), 117-130. https://doi.org/10.23938/ASSN.0059
[27] Jassi, F. J., & Paschoal, L. H. C. (2011). Terapia manual no tratamento da espondilólise e espondilolistese: revisão de literatura [Manual therapy for treating spondylolysis and spondylolisthesis: a literature review]. Revista Brasileira de Ciências da Saúde, 9(27), 59-66.
[28] Ferrari, S., et al. (2012). Clinical presentation and physiotherapy treatment of 4 patients with low back pain and isthmic spondylolisthesis. Journal of Chiropractic Medicine, 11(2), 94-103. https://doi.org/10.1016/J.JCM.2011.11.001
[29] Pristianto, A. (2023). Program Fisioterapi Pada Kondisi Low Back Pain Et Causa Spondylolisthesis: Laporan Kasus [Physiotherapy Program for Low Back Pain Due to Spondylolisthesis: A Case Report]. Tirtayasa Medical Journal, 2(2), 1-10. https://doi.org/10.52742/tmj.v2i2.19532
[30] Garet, M., et al. (2013). Nonoperative treatment in lumbar spondylolysis and spondylolisthesis: a systematic review. Sports Health: A Multidisciplinary Approach, 5(3), 225-232. https://doi.org/10.1177/1941738113480936
ごあいさつ

長引いた痛みを一人で治すのは困難なことが多いです。
困ったときは自身で判断せずに適切な処置を受けるために専門家に相談しましょう。
もし、お近くにお住まいで、困っているならば、一度ひまわり接骨院までお問い合わせください。腰痛・坐骨神経痛の専門家の新幡が、ご相談に乗ります。
気軽にご相談ください。

新着情報・お知らせ
お気軽にお問合せください

お電話でのお問合せ・相談予約
<受付時間>
月~土
9:00〜13:00 /15:00〜19:00
※日曜・祝日は除く
フォームは24時間受付中です。お気軽にご連絡ください。
ひまわり接骨院

住所
〒213-0002
神奈川県川崎市高津区二子1丁目7−17 リバーサイドマンション杉崎 102
アクセス
二子新地駅 徒歩3分
駐車場:近隣にコインパーキングあり。自転車・バイクは店舗前に駐輪場がございます。
受付時間
月~土
9:00〜13:00 /15:00〜19:00
定休日
日曜・祝日

