
〒213-0002 神奈川県川崎市高津区二子1丁目7−17
リバーサイドマンション杉崎 102 二子新地駅 徒歩3分
| 月 | 火 | 水 | 木 | 金 | 土 | 日祝 | |
|---|---|---|---|---|---|---|---|
| 9:00〜13:00 | ● | ● | ● | ● | ● | ● | ─ |
| 15:00〜19:00 | ● | ● | ● | ● | ● | ● | ─ |
手術タイミングと判断基準:二次性変形性股関節症
公開日:2026/05/14
更新日:2026/00/00
二次性変形性股関節症(先天的な股関節の形成不全(臼蓋形成不全など)や過去のケガ・病気が原因で、軟骨がすり減り、股関節の変形が進む病気で,原因がはっきりとしているも)の患者が適切な治療法を選択するための科学的根拠に基づいた意思決定支援ガイドです。
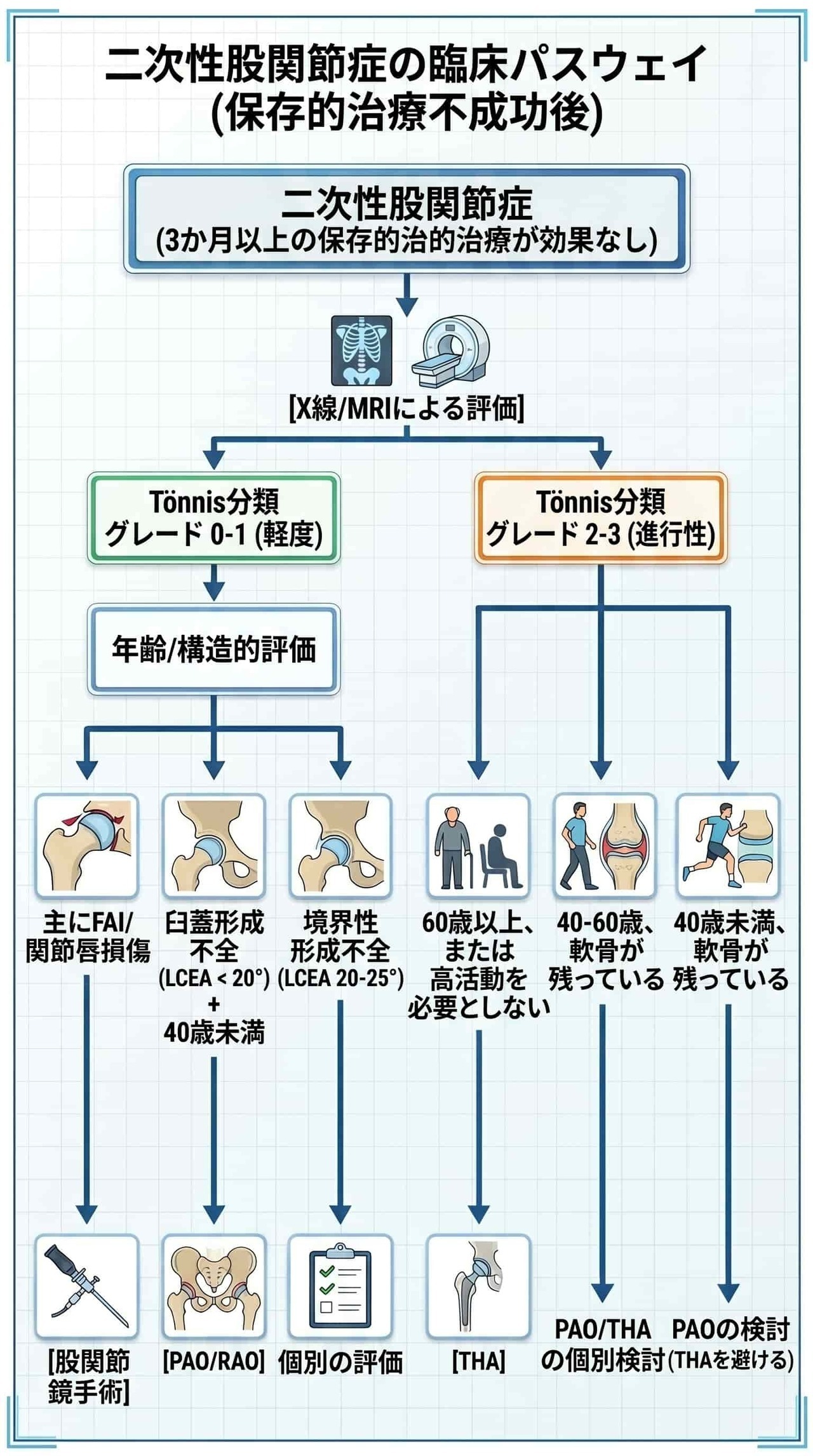
まず、保存療法を少なくとも3ヶ月継続しても日常生活に支障がある場合に手術を検討すべきという基本原則が示されています。
手術の選択肢として、関節を温存する骨切り術や股関節鏡手術、進行期に適した人工股関節全置換術(THA)の3種が挙げられ、それぞれの適応基準が詳しく解説されています。
術式の決定には、年齢や関節の変形度合いといった物理的要因だけでなく、糖尿病や肥満などの合併症リスクも考慮する必要があります。
最終的に、最新のエビデンスと個人の価値観を照らし合わせ、医師と患者が対話を通じて方針を決める共同意思決定の重要性を説いています。本書は、最適な手術タイミングを逃さず、患者の**生活の質(QOL)**を最大化するための実用的な指針となっています。
二次性変形性股関節症とは、加齢や肥満などが主な原因となる「一次性」とは異なり、股関節の構造的な異常(基礎疾患)が原因となって関節軟骨がすり減り、痛みや機能障害を引き起こす疾患です。
股関節の「受け皿」となる寛骨臼の発育が不十分で、大腿骨頭(太ももの骨の先端)の被覆が浅い状態です。この形態異常によって股関節の不安定性が増し、局所的に高い接触圧がかかるようになるため、関節軟骨の変性が進んで変形性関節症へと進行してしまいます。
大腿骨頭・頸部と寛骨臼の形態に異常があることで、股関節を曲げたり回転させたりする際に、骨同士の異常な衝突(インピンジメント)が生じる病態です。大腿骨側に異常がある「cam型」、寛骨臼側に異常がある「pincer型」、またはその両方が合併した「混合型」があり、衝突の繰り返しによって軟骨や関節唇が損傷します。
参考文献によると、二次性変形性股関節症の手術療法には、大きく分けて以下の3つの選択肢があります。
- 特徴: 進行した変形性股関節症に対する最も一般的で効果的な手術です。傷んだ関節を人工物に置き換えることで、確実な痛みの軽減と機能の改善が期待でき、術後早期から良好な機能回復が得られます。
- 適応となる方: 一般的に60歳以上の方や、変形性関節症が進行している(関節裂隙が2mm以下など)方に推奨されることが多いです。
- 特徴: 患者さん自身の関節を温存しながら治療する「関節温存手術」です。骨盤の骨を切って寛骨臼(股関節の受け皿)の向きを変えることで、大腿骨頭の被覆を改善し、関節にかかる負担を軽減します。代表的な術式として、ベルン寛骨臼回転骨切り術(PAO)と回転寛骨臼骨切り術(RAO)があります。
- 適応となる方: 比較的若年(主に40歳未満)から中年の方で、関節軟骨の損傷が軽度であり、自身の関節を長期間温存したい方に推奨されます。年齢よりも術前の関節の状態が重要視されます。
- 特徴: 大腿骨寛骨臼インピンジメント(FAI)などによる二次性変形性股関節症に対する、体への負担が少ない低侵襲な手術です。関節を大きく切開せず、小さな切開から内視鏡を入れて関節内の処置(骨の形態修正や損傷した関節唇の修復など)を行い、痛みの軽減を目指します。
- 適応となる方: 症状があり、画像検査でインピンジメントの証拠が確認され、3〜6ヶ月程度の保存療法(理学療法など)を行っても効果が不十分であった方に検討されます。変形性関節症の進行が軽度であることが重要です。
最適な手術の選択肢は、患者さんの年齢、活動レベル、関節の変性の程度、基礎疾患の種類、ご自身の希望や価値観などを総合的に考慮し、担当医と十分に話し合った上で決定されます。
人工股関節全置換術(THA)、骨切り術、股関節鏡手術の使い分けは、主に**「年齢」「変形性関節症の進行度」「原因となっている基礎疾患」「患者さん自身の希望」**という4つの要素を総合的に評価して決定されます。
- 40歳未満: 若年層では、自身の関節を残す関節温存手術(骨切り術または股関節鏡)が第一選択となることが多くなります。
- 40〜60歳: 関節温存手術とTHAのどちらも適応となり得る**「境界領域」**です。術前の関節の状態が良好であれば関節温存も可能ですが、年齢が上がるにつれて関節温存手術の失敗リスクが上昇するため、生活様式などを踏まえた個別の検討が必要です。
- 60歳以上: 一般的に、確実な痛みからの解放と早期の機能回復が期待できる人工股関節全置換術(THA)が第一選択として推奨されます。
進行度は画像所見(Tönnis分類など)を用いて判断されます。
- 軽度(Tönnis分類グレード0〜1): 関節軟骨の損傷が軽度であるため、**関節温存手術(骨切り術や股関節鏡)**の適応となります。
- 中等度(Tönnis分類グレード2): 治療選択が難しい領域です。この段階で骨切り術や股関節鏡を行うと失敗リスクが高まる(骨切り術では失敗リスクが3.36倍になるなど)ため、THAを選択することが合理的な判断とされています。
- 進行期(Tönnis分類グレード3、関節裂隙2mm以下): 関節温存手術は推奨されず、THAが主な選択肢となります。
年齢や進行度から「関節温存手術」が適していると判断された場合、原因疾患によって術式が分かれます。
- 明らかな股関節形成不全(LCEA 20度未満): 股関節の受け皿が浅いことが原因の場合は、骨盤を切って被覆を改善する骨切り術が推奨されます。
- 大腿骨寛骨臼インピンジメント(FAI): 骨の形態異常による衝突(インピンジメント)が原因であり、3〜6ヶ月の保存療法で効果が不十分な場合は、骨の形態修正等を行う股関節鏡手術を検討します。
- ※境界型形成不全(LCEA 20〜25度): 判断が非常に難しい領域であり、股関節鏡手術よりも骨切り術の方が良好な成績が得られるという報告もあるため、個別の詳細な評価が必要です。
- 若年で活動的であり、**「どうしても自分の関節を残したい」**という強い希望がある場合は、変形性関節症が軽度であることを条件に関節温存手術が適しています。
- 活動レベルにかかわらず、**「確実な痛みの軽減」**を最優先とする場合は、THAの方が優れた除痛効果を期待できます。
このように、単一の基準ではなく、これらの要素を掛け合わせて「早すぎず、遅すぎない」適切なタイミングで術式を選択することが重要とされています。
人工股関節全置換術(THA)の適応と禁忌は、痛みや機能障害、画像所見、保存療法の効果などを総合的に評価して以下のように判断されます。
- 症状と機能障害: 痛み、可動域の制限、歩行距離の制限、そして患者さん自身が感じる苦痛が最も重要な指標となります。
- 保存療法の限界: 理学療法や鎮痛薬などの保存療法を試みても十分な効果が得られなかった場合、さらなる保存療法を追加するよりもTHAへの移行を検討すべきとされています。
- 画像所見: 進行した変形性股関節症が主な対象です。一方で、画像所見が軽度な段階では手術による臨床的な改善が実感しにくいため、THAを急ぐべきではないとされています。
- 年齢: 年齢そのものは絶対的な基準ではなく、適切な評価と管理を行えば、若年者から高齢者まで実施可能です。
- 遅らせるべき状況: 喫煙習慣のある方(禁煙のため)や糖尿病の方(血糖コントロール改善のため)は、術後の合併症リスクを減らす目的で手術を遅らせることが推奨されます。
- 遅らせるべきでない状況: 重度の変形や骨欠損、神経障害性関節症がある場合は、保存療法を続けることで状態がさらに悪化するリスクがあるため、手術を遅らせるべきではありません。
- 活動性の感染: 股関節に化膿性関節炎などの感染がある状態で行うと、人工関節周囲感染のリスクが極めて高くなります。
- 重度の全身状態不良: 麻酔や手術自体に耐えられない状態。
- 歩行能力の欠如: 自力での歩行能力がない患者さんの場合、THAによる機能改善の効果が限定的となるため、通常は適応外となります。
- 肥満: BMIの上昇に伴って合併症リスクが直線的に高くなります。
- 高齢: 年齢とともに合併症リスクは増加しますが、術前状態が管理されていれば生活の質の大幅な改善が期待できます。
- 併存疾患: 糖尿病(感染リスクの増加)、慢性腎臓病(死亡や再入院リスクの増加、透析中で移植待機中の場合は移植後までの延期を推奨)、心臓弁膜症などの心疾患(急性心イベントリスクの増加)。
- その他: 栄養不良(低アルブミン血症など)や喫煙も、術後合併症のリスク因子となります。
最終的な適応とタイミングは、これらの医学的な基準とあわせて、ご自身の希望や生活背景を担当医と十分に話し合った上で決定されます。
骨切り術(PAO/RAO)は、患者さん自身の関節を温存しながら股関節にかかる負担を軽減することを目的とした「関節温存手術」です。この手術の適応と禁忌については、主に年齢、関節の変性度、および股関節形成不全の程度に基づいて判断されます。
- 変形性関節症の進行度(最も重要な因子) 手術の成否を左右する最大の要因は、術前の変形性関節症の進行度です。関節軟骨の損傷が軽度である「Tönnis分類グレード0または1(前期・初期)」の段階が理想的な適応とされます。
- 年齢 主に若年から中年の患者さんが対象です。従来は40歳以上は適応外とされることが多かったですが、最近の研究では年齢そのものよりも「術前の関節の状態」が重要視されています。変形が軽度で機能が良好であれば、40歳以上でも良好な成績が期待できます。ただし、年齢が高いほど手術失敗のリスクは上昇する傾向にあります。
- 股関節形成不全の程度 X線画像で測定される外側中心縁角(LCEA)が20度未満の「明らかな股関節形成不全」と診断された場合が骨切り術の適応となります。なお、LCEAが20〜25度の「境界型形成不全」は判断が難しい領域ですが、股関節鏡手術よりも骨切り術の方が良好な成績が得られるという報告があります。
- その他の必須条件 股関節形成不全があっても無症状の場合は適応となりません。痛みや機能障害があり、日常生活に支障をきたしていることが前提です。また、股関節を外側へ開いた際(外転時)に大腿骨頭と寛骨臼の適合性が改善し、関節裂隙が広がる(関節適合性が保たれている)こと、良好な可動域があることも重要な適応基準となります。
- Y軟骨の開存: 成長期の患者さんでY軟骨(三放軟骨)が開存している場合は手術できず、閉鎖するまで待つ必要があります。
- 進行した変形性関節症: Tönnis分類グレード2を超える進行した変形性関節症では、長期間の関節温存が難しいため適応外となり、人工股関節全置換術(THA)を検討すべきとされます。
- 末期変形性関節症: 関節裂隙が完全に消失している状態。
- 高位脱臼や二次性寛骨臼。
- リウマチ性関節炎。
- Tönnis分類グレード2の変形性関節症: 手術成績が不良になる可能性が高いため、患者さんが自身の関節を残すことを強く希望し、十分な説明と同意があった場合などに検討されます。
- 肥満: BMIが高い(例:24 kg/m²を超えるなど)患者さんでは、手術失敗や将来的なTHAへの移行リスクが高くなります。
- 術前の関節適合性不良: X線で股関節を外転させても適合性が改善しない、または関節裂隙が広がらない場合は適応外となります。
- 40歳以上の年齢: 関節の状態が良い場合は手術可能ですが、相対的禁忌として慎重に評価されることがあります。
股関節鏡手術は、関節を大きく切開せず小さな切開から内視鏡を入れて処置を行う低侵襲な手術であり、主に大腿骨寛骨臼インピンジメント(FAI)による二次性変形性股関節症に対して行われます。適応と禁忌の基準は以下の通りです。
基本的な適応条件は、症状があり、画像検査でインピンジメントの証拠が確認され、3〜6ヶ月程度の保存療法を試みても効果が不十分であった患者さんです。
- 変形性関節症の進行度: 関節の変性が軽度であること(Tönnis分類グレード0または1)。
- 年齢: 45歳以下であること。
- 症状の持続期間: 症状が現れてから2年未満であること。症状が2年未満の患者さんは、2年以上の患者さんと比較して人工関節への移行率や再手術率が低く、術後の成績が良好であることが報告されています。
- 進行した変形性関節症: 関節裂隙が2mm以下、またはTönnis分類グレード2を超える進行した変形性関節症の場合、股関節鏡手術の効果が得られにくく、人工股関節全置換術(THA)への移行が必要となる可能性が高いため、禁忌(慎重な判断が必要)とされています。このような患者さんではTHAを検討すべきです。
- 年齢: 45歳を超える年齢。
- 症状の持続期間: 症状が2年以上続いている場合。
- 関節の状態: 大きな寛骨臼軟骨欠損がある場合。
- 境界型形成不全: 股関節の受け皿の被覆を示す外側中心縁角(LCEA)が20〜25度の「境界型形成不全」の患者さんでは、股関節鏡手術よりも骨切り術の方が良好な成績が得られるという報告があるため、骨切り術の方が適している可能性があります。
二次性変形性股関節症の手術を検討する際の基本的な考え方は、**「早すぎず、遅すぎず」**です。一般的に、適切な保存療法(理学療法や鎮痛薬など)を少なくとも3ヶ月以上継続しても十分な効果が得られず、日常生活に大きな支障がある場合に手術のタイミングとして検討されます。
- 保存療法が限界に達した時が検討のタイミングです。中等度から重度の変形性股関節症において保存療法が効果的でない場合、さらに別の保存療法(注射や歩行補助具など)を追加するためにTHAを遅らせることは推奨されていません。
- 手術を遅らせるべきケース: 喫煙習慣のある方は禁煙やニコチン減量のため、糖尿病の方は血糖コントロールを改善するために手術を遅らせることが推奨されます。
- 遅らせるべきでないケース: 重度の変形や骨欠損、神経障害性関節症がある場合は、保存療法を続けることで状態がさらに悪化するリスクがあるため、手術を遅らせるべきではありません。
- 早すぎる手術への注意: 画像所見上の変形が軽度な段階では、手術による臨床的な改善が実感しにくいため、THAを急ぐべきではありません。最終的なタイミングは、患者さん自身の苦痛の程度に基づいて決定されます。
- 骨切り術の成功には**「機会の窓(最適なタイミング)」**という概念が非常に重要です。
- 関節の変性が進行してしまうと適応がなくなり、人工股関節置換術しか選択肢がなくなってしまうため、変形性関節症が進行する前の「早期」に手術を行うことが推奨されています。
- 一方で、画像所見が軽度な段階で手術を行うと、手術による改善の余地が少ないため臨床的に意味のある改善が得られにくいという報告もあります。症状の程度と手術のリスク・利益のバランスを考慮してタイミングを見極める必要があります。
- 3〜6ヶ月間の保存療法を試みても効果が不十分な場合に、手術のタイミングとして検討されます。
- 症状の持続期間が短いほど、手術成績が良好になります。具体的には、症状の発現から「2年未満」の患者さんは、「2年以上」経過している患者さんと比較して、術後の機能スコアが高く、人工関節への移行率(0.6%対6.4%)や再手術率(0.9%対10.1%)も低いことが報告されています。
- したがって、保存療法が効果的でない場合には、我慢しすぎずに早期に手術を検討することが推奨されます。
手術の最適なタイミングは、同じ画像所見や年齢であっても、患者さんの活動レベル、職業、生活様式、ご自身の希望によって異なります。
担当医と各治療法の利点と欠点について十分に話し合い(共同意思決定)、ご自身が納得できるタイミングを選択することが最も重要です。
参考文献に基づき、人工股関節全置換術(THA)、骨切り術(PAO/RAO)、股関節鏡手術の長期成績と生存率(自分の関節を温存できた割合)について解説します。
- 理想的な条件(40歳未満、関節変性が軽度など)の場合: 5年生存率は96%、10年生存率は91%、15年生存率は85%、**20年生存率は68%**と報告されています。
- 別の大規模調査: 10年生存率が約75.9%、20年生存率が約36.5%とする報告もあります。
- 30年追跡調査: 手術から30年経過した時点で、29%の股関節が温存されていました。残りの70%以上は、変形性関節症が進行したり、THAへ移行したりしました。
- 変形性関節症「前期」: 10年・20年生存率ともに96%、**30年生存率は81.8%**と非常に良好です。
- 変形性関節症「初期」: 10年生存率89%、20年生存率78%、**30年生存率は42.2%**となります。
- 変形性関節症「進行期」: 20年後の関節温存率が59.3%にまで低下し、20年以内に34%の患者さんがTHAに移行しました。
- 症状の持続期間による違い:
- 症状が始まってから**「2年未満」**の患者さんでは、THAへの移行率が0.6%、再手術率が0.9%と極めて低く良好です。
- 一方、症状が**「2年以上」**続いている患者さんでは、THAへの移行率が6.4%、再手術率が10.1%と悪化します。
- 関節症が進行している場合:
- 中等度から進行した変形性関節症(Tönnis分類グレード2または3)の患者さんでは、一時的な改善は見られても、平均18ヶ月後に44%の患者さんがTHAを必要としたという厳しい報告があります。
- 中等度から進行した変形性関節症(Tönnis分類グレード2または3)の患者さんでは、一時的な改善は見られても、平均18ヶ月後に44%の患者さんがTHAを必要としたという厳しい報告があります。
- その他の追跡調査: 英国の試験(FASHIoN試験)では、手術後3年以内に2%の患者がTHAを受け、12%が再鏡視術(再手術)を受けたと報告されています。
- 確実性と長期安定性を求める場合はTHAが優れています。
- 自分の関節を残す骨切り術や股関節鏡手術で良好な長期成績(生存率)を得るためには、「変形性関節症が進行する前の、条件が良い早期の段階」で手術のタイミングを逃さないことが最も重要になります。
参考文献に基づいて、各術式(人工股関節全置換術、骨切り術、股関節鏡手術)における手術不適応(手術できない、またはすべきでない基準)をまとめます。
不適応の基準には、手術を絶対に行うべきでない「絶対的禁忌」と、リスクが高いため慎重な判断が必要となる「相対的禁忌」があります。
- 活動性感染: 股関節に化膿性関節炎などの活動性感染がある場合、人工関節周囲感染のリスクが極めて高くなるため絶対的禁忌です。
- 重度の全身状態不良: 麻酔や手術自体に耐えられない状態。
- 歩行能力の欠如: 自力での歩行能力がない患者さんの場合、THAによる機能改善の効果が限定的となるため、通常は適応外となります。
- 肥満: 特にBMIが40 kg/m²を超える場合、深部感染や再手術などの合併症リスクが著しく高まるため、相対的禁忌と位置づけられることがあります。
- 併存疾患: コントロールされていない糖尿病(感染リスク増)、慢性腎臓病(特に透析中や移植待機中の場合)、心臓弁膜症などの心疾患は合併症リスクを高めます。
- その他: 栄養不良(低アルブミン血症)や喫煙も合併症のリスク因子となります。喫煙者や糖尿病患者さんに対しては、状態を改善させるため(禁煙や血糖コントロール)に手術を遅らせることが推奨されています。
- Y軟骨の開存: 骨切り術は骨盤の骨(Y軟骨)を横切るため、成長期でY軟骨が閉鎖していない患者さんには適用できません。
- 進行した変形性関節症: Tönnis分類グレード2を超える進行した変形性関節症や、関節裂隙が完全に消失した末期変形性関節症の場合、関節を長期間温存できる可能性が低いため適応外となります。
- その他: 高位脱臼や二次性寛骨臼、リウマチ性関節炎による股関節症も絶対的禁忌です。
- 年齢と進行度: 40歳以上の年齢や、Tönnis分類グレード2の変形性関節症は手術成績が不良となるリスクがあるため、慎重な判断が必要です。
- 関節の適合性不良: X線で股関節を外側に開いた際(外転時)に関節の適合性が改善しない、または関節の隙間が広がらない場合は適応外となります。
- 肥満: BMIが高い患者さんでは、手術失敗のリスクが高くなります。
- 進行した変形性関節症: 関節の隙間(関節裂隙)が2mm以下、またはTönnis分類グレード2を超える進行した変形性関節症の場合、手術の効果が得られにくく人工関節への移行リスクが高いため、THAを検討すべきとされています。
- 症状の持続期間と年齢: 症状が「2年以上」続いている場合や、「45歳を超える」年齢は、手術成績が不良となるリスク因子とされています。
- 関節の構造的な問題: 大きな寛骨臼軟骨欠損がある場合もリスク因子です。また、股関節の受け皿の被覆を示すLCEAが20〜25度の「境界型形成不全」の場合、股関節鏡手術よりも骨切り術の方が良好な成績が得られるという報告があるため、骨切り術の方が適している可能性があります。
参考文献には、各術式の「具体的なリハビリ期間(何ヶ月など)」や「具体的な動作の制限事項(してはいけない姿勢など)」に関する詳細な記載はありません。
しかし、術後の機能回復の早さや、活動制限の程度に関する術式ごとの特徴については、以下の通り記載されています。
- 術後の生活制限: 活動制限の有無とその程度
- 社会復帰の時期: 仕事や趣味への復帰にかかる期間
- リハビリテーション: 具体的な内容と期間
参考文献に基づき、各術式における「手術失敗(成績不良、合併症の発生、次の手術への移行など)」のリスクを高める予測因子について解説します。
- 肥満: BMIの増加に伴って合併症リスクが直線的に上昇します。特にBMIが40 kg/m²を超える場合、深部感染や再手術のリスクが非常に高くなります。
- 併存疾患:
- 糖尿病: 手術部位や尿路・下気道などの感染リスクが有意に高くなります。
- 慢性腎臓病: 特にステージ3以上や透析中の患者さんでは、死亡や再入院、脱臼、人工関節周囲感染のリスクが高く、予後不良の重要な予測因子となります。
- 心疾患: 心臓弁膜症などがある場合、急性心イベントや死亡率のリスクが高くなります。
- 栄養不良: 低アルブミン血症(血清アルブミン<3.4 g/L)は、病的肥満よりも独立した合併症の予測因子とされています。
- 喫煙: 全原因による再置換リスクや人工関節周囲感染のリスクを増加させる因子です。
- 高齢: 年齢の増加に伴い心合併症などのリスクが上昇します。
- 変形性関節症の進行度(最も重要): 術前のTönnis分類グレードが高い(グレード2以上)ほど、手術失敗のリスクが著しく高くなります。
- 年齢: 手術時年齢が高い(特に40歳や46歳以上)ほど、関節症の進行やTHAへの移行リスクが高まります。
- 術前の機能と症状: 術前の機能スコア(Merle d'Aubigne-Postelスコアなど)が低い、あるいは術前に跛行がある場合、失敗リスクが高くなります。
- 股関節形成不全の重症度: 外側中心縁角(LCEA)が0度未満の場合。
- 肥満: BMIが30 kg/m²以上(または24 kg/m²を超える場合)は、失敗やTHAへの移行リスクが高くなります。
- 前方インピンジメントテスト陽性: 術前にこのテストが陽性の場合もリスク因子です。
- 被覆の過不足: 術後のLCEAが30度未満(被覆不足)または40度を超える(過剰被覆)場合。
- 関節適合性の不良: 術後の関節適合性が悪いと、変形性関節症の進行リスクが著しく(12.1倍に)高まるという報告があります。
- その他の要因: 術後に寛骨臼後方開放が生じた場合や、異所性骨化が形成された場合も失敗のリスクが高くなります。
- 変形性関節症の進行度: Tönnis分類グレード1以上、または関節裂隙が2mm以下の患者さんでは、手術の効果が得られにくくTHAへ移行する可能性が高くなります。
- 症状の持続期間: 症状が現れてから「2年以上」経過している場合、術後の成績が不良となり、再手術率やTHAへの移行率が高くなることが報告されています。
- 年齢: 45歳を超える患者さんでは、術後の臨床成績が不良となるリスクが高まります。
- 関節の状態: 大きな寛骨臼軟骨欠損がある場合も、成績不良となるリスク因子とされています。
いずれの手術においても、**「関節の変性が進行していること」と「肥満などの全身的なリスク因子があること」**が共通して失敗や合併症の予測因子となっています。
これらの因子を事前に正しく評価し、必要に応じて体重減量や禁煙などの「術前最適化」を行うことが、手術を成功に導くために非常に重要です。
手術(特に人工股関節全置換術:THA)を遅らせるべき状況は、主に術後の合併症リスクを減らすための**「術前最適化」が必要なケース**です。ガイドラインなどで推奨されている具体的な状況は以下の通りです。
- 喫煙している場合: ニコチンの減量や禁煙を行うために、手術を遅らせることが条件付きで推奨されています。
- 糖尿病がある場合: 術後の感染リスクなどを減らすため、血糖コントロールを改善させる目的で手術を遅らせることが条件付きで推奨されています(具体的な指標や目標値は示されていません)。
- 透析中で移植待機中の場合: 慢性腎臓病で透析を受けており、かつ腎移植の待機リストに登録されている患者さんでは、合併症リスクが非常に高いため、腎移植が終わるまでTHAを延期することが推奨されています。
- 重度の関節の変形がある場合。
- 重度の骨欠損がある場合。
- 神経障害性関節症の患者さんの場合。
各手術における長期的な見通し(自身の関節がどれくらい温存できるか、将来的に人工股関節全置換術:THAが必要になる可能性)は、**「手術を受ける前の関節の進行度」**に最も大きく左右されます。
骨切り術は関節の温存を目的としますが、術後の経過年数や術前の状態によってTHAが必要になる(関節温存に失敗する)割合が変わります。
- 関節温存期間(生存率)の目安:
- ベルン寛骨臼回転骨切り術(PAO): 理想的な条件(若年で変形が軽度など)で行われた場合、10年生存率は約76%〜91%、20年生存率は約37%〜68%と報告されています。30年後では、約29%の患者さんが関節を温存できていました。
- 回転寛骨臼骨切り術(RAO): 術前の病期によって明確な差があります。変形性関節症が「前期」の段階で手術を受けると、30年後でも約81.8%の方が関節を温存できています。しかし「初期」の段階では30年生存率が約42.2%に低下し、「進行期」では20年以内に34%がTHAに移行したと報告されています。
- ベルン寛骨臼回転骨切り術(PAO): 理想的な条件(若年で変形が軽度など)で行われた場合、10年生存率は約76%〜91%、20年生存率は約37%〜68%と報告されています。30年後では、約29%の患者さんが関節を温存できていました。
- THAへの移行時期:
- ある研究では、骨切り術後にTHAへの移行が必要になった時期は、術前の病期が「前期」だった場合は平均23年後、「初期」では平均14.5年後、「進行期」では平均13.7年後でした。
- つまり、変形が少ない早期に手術を受けるほど、数十年単位で自分の関節を長く残せる可能性が高まります。
- ある研究では、骨切り術後にTHAへの移行が必要になった時期は、術前の病期が「前期」だった場合は平均23年後、「初期」では平均14.5年後、「進行期」では平均13.7年後でした。
股関節鏡手術後の長期的な見通しは、主に「症状がどのくらいの期間続いていたか」と「関節の変性の進行度」に依存します。
- 症状の持続期間によるTHAへの移行率:
- 症状が現れてから**「2年未満」**で手術を受けた患者さんは、THAへの移行率がわずか0.6%、再手術率も0.9%と非常に良好な見通しが示されています。
- 一方、症状が**「2年以上」**続いていた患者さんは、THAへの移行率が6.4%、再手術率が10.1%と悪化します。
- 進行した変形性関節症の場合:
- すでに中等度から進行した変形性関節症(Tönnis分類グレード2または3)の患者さんの場合、一時的な改善は見られても、平均18ヶ月後には約44%の患者さんがTHAを必要としたという厳しいデータがあります。
THAは自身の関節を温存する手術ではありませんが、進行した変形性関節症に対する「最終的な治療」として非常に安定した長期成績を持ちます。
- 現代のインプラントを用いた場合、20歳以下の若年患者さんであっても、中期から長期にわたって良好な臨床成績とインプラントの生存率が期待できます。
- 高齢の患者さんや併存疾患がある患者さんでも、適切な術前評価と管理を行えば、安全かつ長期的に大幅な生活の質の改善がもたらされます。
- 痛みを確実に取り除き、長期的な安定を求める場合はTHAが最も確実な選択肢です。
- 自分の関節を残す(骨切り術や股関節鏡手術)ことを希望し、将来的なTHAの必要性を可能な限り低くしたい場合は、関節の変性が進んでしまう前の**「早期(機会の窓)」に手術のタイミングを逃さないこと**が何よりも重要です。
術前最適化(手術前の状態改善)として具体的に行うべき取り組みには、主に以下の「修正可能なリスク因子」に対する介入が含まれます。
- 禁煙・ニコチンの減量 喫煙は人工関節周囲感染や再置換のリスクを増加させるため、手術前に禁煙またはニコチンの減量を行うことが条件付きで推奨されています。
- 血糖コントロールの改善 糖尿病は手術部位や尿路・下気道などの感染リスクを有意に高めるため、事前に血糖コントロールを改善させることが推奨されています(ただし、具体的な指標や目標値はガイドライン等では示されていません)。
- 体重管理・減量の試み 肥満(特にBMIが高い場合)は合併症リスクを上昇させます。BMIが30 kg/m²を超える場合は減量の試みが推奨されており、BMIが40 kg/m²を超える高度肥満の患者さんでは、選択的手術の前に肥満専門医へ紹介して減量を図るべきとする報告もあります。ただし、BMIのみを理由に手術を拒否するのではなく、他の要因も含めた個別化されたリスク評価が重要視されています。
- 栄養状態の評価と改善 低アルブミン血症(血清アルブミン<3.4 g/L)に代表される栄養不良は、病的肥満以上に合併症の独立した予測因子となるため、事前の栄養状態の評価と改善が重要です。
- 腎移植の優先(該当する透析患者さんの場合) 慢性腎臓病で透析を受けており、かつ腎移植の待機リストに登録されている患者さんの場合は、手術の合併症リスク・死亡率が極めて高いため、腎移植が終わるまで手術(THAなど)を延期することが推奨されます。
- 高容量外科医(年間手術件数の多い医師)への紹介の検討 病的肥満などのハイリスク患者さんにおいては、手術経験が豊富な(年間実施数が多い)外科医に手術を依頼することで、合併症リスクの低減と良好な成績が期待できるとされています。
保存療法(非手術的治療)の限界に達したと判断し、手術療法への移行を検討する際の主な基準は以下の通りです。
適切な保存療法を一定期間継続しても、患者さんの痛みや機能障害が十分に改善しないことが最も重要な指標となります。具体的な試行期間の目安として、進行した変形性股関節症の場合は**「少なくとも3ヶ月間」、大腿骨寛骨臼インピンジメント(FAI)の場合は「3〜6ヶ月間」**の保存療法を継続して反応しない場合、保存療法の限界と判断され手術が検討されます。
すでに効果が不十分な患者さんに対して、理学療法、鎮痛薬(NSAIDs)、歩行補助具、関節内注射などの追加的な保存療法を行うことだけを目的として手術(特に人工股関節全置換術:THAなど)を遅らせることは推奨されていません。効果が出ていない状況で漫然と保存療法を追加しても、さらなる改善が得られにくいことを示唆しています。
保存療法を継続しても、痛みのために仕事、家事、趣味などの日常活動が大きく制限され、生活の質が著しく低下していることも重要な判断基準です。各種ガイドラインでも、痛みや機能といった患者さんにとって重要なアウトカムの改善を目的として手術のタイミングを決定すべきとしています。
限界を判断する客観的な指標として、患者さんが自身の状態を回答するPROスコアも用いられます。研究によれば、理学療法を受けた患者さんのうち、臨床的に意味のある改善(MCID)や、患者さんが許容できる症状状態(PASS)の基準に達する割合は2割〜3割程度にとどまるという結果が出ており、これが保存療法単独の限界を示す根拠となっています。
X線などの画像所見の進行も考慮すべき要因です。画像上で関節軟骨の損傷や関節症が進行してしまった状態では、関節温存手術の適応から外れてしまい、人工関節置換術しか選択肢がなくなるため、病期の進行自体が保存療法の限界を示します。
実際に、保存療法(理学療法など)を選択した患者さんの一定割合(研究によっては24%から最大70%)が、最終的に手術を選択しているというデータもあります。したがって、3〜6ヶ月程度適切な保存療法を行っても日常生活に支障をきたすような症状が残る場合は、限界と見なして手術を前向きに検討する段階と言えます。
[1]C. P. Hannon, R. E. Delanois, S. Nandi, and Y. A. Fillingham, “American Academy of Orthopaedic Surgeons Clinical Practice Guideline Summary Management of Osteoarthritis of the Hip.,” Journal of The American Academy of Orthopaedic Surgeons, May 2024, doi: 10.5435/jaaos-d-24-00420.
[2]A. Postler, C. Lützner, J. Goronzy, S. Deckert, and K.-P. Günther, “When are patients with osteoarthritis referred for surgery?,” Best Practice & Research: Clinical Rheumatology, pp. 101835–101835, May 2023, doi: 10.1016/j.berh.2023.101835.
[3]R. H. Quinn, J. Murray, R. Pezold, and Q. Hall, “Management of Osteoarthritis of the Hip.,” Journal of The American Academy of Orthopaedic Surgeons, vol. 26, no. 20, Oct. 2018, doi: 10.5435/JAAOS-D-18-00351.
[4]T. R. McCarroll, B. D. Kuhns, and B. G. Domb, “Surgical Management of Hip Pain in Active Patients With Early Osteoarthritis: Navigating the Choice Between Hip Preservation and Arthroplasty,” Journal of The American Academy of Orthopaedic Surgeons, Dec. 2024, doi: 10.5435/jaaos-d-24-00242.
[5]F. Atsma, O. Molenkamp, H. Bouma, S. B. Bolder, A. S. Groenewoud, and G. P. Westert, “Uniform Criteria for Total Hip Replacement Surgery in Patients With Hip Osteoarthritis; a Decision Tool to Guide Treatment Decisions.,” International Journal for Quality in Health Care, vol. 33, no. 1, Mar. 2021, doi: 10.1093/INTQHC/MZAB030.
[6]G. A. Hawker, “The Devil Is in the Detail: Clinical Practice Guideline for the Optimal Timing of Elective Hip or Knee Arthroplasty,” Arthritis & rheumatology, vol. 75, July 2023, doi: 10.1002/art.42659.
[7]C. P. Hannon et al., “2023 American College of Rheumatology and American Association of Hip and Knee Surgeons Clinical Practice Guideline for the Optimal Timing of Elective Hip or Knee Arthroplasty for Patients With Symptomatic Moderate-to-Severe Osteoarthritis or Advanced Symptomatic Osteonecrosis With Secondary Arthritis for Whom Nonoperative Therapy Is Ineffective,” Journal of Arthroplasty, vol. 38, no. 11, pp. 2193–2201, Nov. 2023, doi: 10.1016/j.arth.2023.09.003.
[8]N. S. Piuzzi, P. A. Manner, and B. R. Levine, “American Academy of Orthopaedic Surgeons Appropriate Use Criteria: Management of Osteoarthritis of the Hip.,” Journal of The American Academy of Orthopaedic Surgeons, vol. 26, no. 20, Oct. 2018, doi: 10.5435/JAAOS-D-18-00335.
[9]H. W. Rees, “Management of Osteoarthritis of the Hip,” Journal of The American Academy of Orthopaedic Surgeons, vol. 28, no. 7, Apr. 2020, doi: 10.5435/JAAOS-D-19-00416.
[10]K. R. Shibata, K. R. Shibata, S. Matsuda, and M. R. Safran, “Open treatment of dysplasia-other than PAO: does it have to be a PAO?,” Journal of Hip Preservation Surgery, vol. 4, no. 2, pp. 131–144, May 2015, doi: 10.1093/JHPS/HNV028.
[11]I. Usiskin, “Surgical Treatments for Osteoarthritis.,” European Journal of Rheumatology, Nov. 2023, doi: 10.5152/eurjrheum.2023.21193.
[12]Akhtar et al., “Patient-Reported Outcomes and Factors Impacting Success of the Periacetabular Osteotomy.,” Cureus, 2023, doi: 10.7759/cureus.37320.
[13]C. P. Hannon et al., “2023 American College of Rheumatology and American Association of Hip and Knee Surgeons Clinical Practice Guideline for the Optimal Timing of Elective Hip or Knee Arthroplasty for Patients With Symptomatic <scp>Moderate‐to‐Severe</scp> Osteoarthritis or Advanced Symptomatic Osteonecrosis With Secondary Arthritis for Whom Nonoperative Therapy Is Ineffective,” Arthritis Care and Research, vol. 75, no. 11, pp. 2227–2238, Sept. 2023, doi: 10.1002/acr.25175.
[14]“Efficacy and safety of arthroscopy in femoroacetabular impingement syndrome: A systematic review and meta-analysis,” Feb. 2023, doi: 10.21203/rs.3.rs-2524433/v1.
[15]N. C. Casartelli, P. L. Valenzuela, N. A. Maffiuletti, and M. Leunig, “Effectiveness of Hip Arthroscopy on Treatment of Femoroacetabular Impingement Syndrome: A Meta-Analysis of Randomized Controlled Trials.,” Arthritis Care and Research, vol. 73, no. 8, pp. 1140–1145, Aug. 2021, doi: 10.1002/ACR.24234.
[16]L. Spencer-Gardner, R. Dissanayake, A. Kalanie, P. J. Singh, and J. O’Donnell, “Hip arthroscopy results in improved patient reported outcomes compared to non-operative management of waitlisted patients.,” Journal of Hip Preservation Surgery, vol. 4, no. 1, pp. 39–44, Jan. 2017, doi: 10.1093/JHPS/HNW051.
[17]A. Realpe et al., “Arthroscopic hip surgery compared with personalised hip therapy in people over 16 years old with femoroacetabular impingement syndrome: UK FASHIoN RCT,” Health Technology Assessment, vol. 26, no. 16, pp. 1–236, Feb. 2022, doi: 10.3310/fxii0508.
[18]M. T. Schwabe et al., “Short-term Clinical Outcomes of Hip Arthroscopy Versus Physical Therapy in Patients With Femoroacetabular Impingement: A Systematic Review and Meta-analysis of Randomized Controlled Trials:,” Orthopaedic Journal of Sports Medicine, vol. 8, no. 11, pp. 2325967120968490–2325967120968490, Nov. 2020, doi: 10.1177/2325967120968490.
[19]N. Ramadanov et al., “Minimal Clinically Important Differences in Conservative Treatment Versus Hip Arthroscopy for Femoroacetabular Impingement Syndrome: A Frequentist Meta‐Analysis of <scp>RCTs</scp>,” Orthopaedic Surgery, July 2025, doi: 10.1111/os.70097.
[20]J. M. Lamo-Espinosa, G. Mariscal, J. Gómez-Álvarez, and M. San-Julián, “Efficacy and safety of arthroscopy in femoroacetabular impingement syndrome: a systematic review and meta-analysis of randomized clinical trials,” Dental science reports, vol. 13, Oct. 2023, doi: 10.1038/s41598-023-43441-y.
[21]G. Anzillotti et al., “Conservative vs. Surgical Management for Femoro-Acetabular Impingement: A Systematic Review of Clinical Evidence,” Stomatology, vol. 11, no. 19, pp. 5852–5852, Oct. 2022, doi: 10.3390/jcm11195852.
[22]P. Robert, H. Robert, D. Dobromir, and B. Roland, “Minimal Clinically Important Differences in Conservative Treatment Versus Hip Arthroscopy for Femoroacetabular Impingement Syndrome: A Frequentist Meta‐Analysis of RCTs,” Nov. 2025, doi: 10.82491/opusthd-33.
[23]M. G. J. Gademan, S. N. Hofstede, T. P. M. V. Vlieland, R. G. H. H. Nelissen, and P. J. M. de Mheen, “Indication criteria for total hip or knee arthroplasty in osteoarthritis: a state-of-the-science overview,” BMC Musculoskeletal Disorders, vol. 17, no. 1, pp. 463–463, Nov. 2016, doi: 10.1186/S12891-016-1325-Z.
[24]J. Dulleston, J. Yoshitani, A. R. R. Fard, and V. Khanduja, “The effect of osteoarthritis grade on patient-reported outcome measures after total hip arthroplasty: a systematic review and meta-analysis,” Orthopaedic proceedings/Journal of bone and joint surgery. British volume. Orthopaedic proceedings, vol. 106-B, no. SUPP_6, pp. 23–23, May 2024, doi: 10.1302/1358-992x.2024.6.023.
[25]M. Li and A. H. Glassman, “What’s New in Hip Replacement.”, doi: 10.2106/jbjs.18.00583.
[26]R. P. Bialaszewski and R. H. Ablove, “The Implications of Obesity on Total Hip Arthroplasties: A Literature Review of the Associated Complications,” Journal of orthopedics and orthopedic surgery, July 2023, doi: 10.29245/2767-5130/2023/2.1184.
[27]D. Mouselimis and C. Lüring, “[Current AWMF Guidelines on Knee and Hip Arthroplasty - Individual Risks].”, doi: 10.1007/s00132-025-04610-1.
[28]E. Jeschke et al., “Obesity Increases the Risk of Postoperative Complications and Revision Rates Following Primary Total Hip Arthroplasty: An Analysis of 131,576 Total Hip Arthroplasty Cases,” Journal of Arthroplasty, vol. 33, no. 7, July 2018, doi: 10.1016/J.ARTH.2018.02.036.
[29]D. Challoumas, N. K. F. K. Ng, T. Altell, S. A. Joiya, J. Horton, and B. Jones, “Outcomes of total hip and knee arthroplasty in special populations: a synopsis and critical appraisal of systematic reviews,” Arthroplasty, vol. 5, no. 1, July 2023, doi: 10.1186/s42836-023-00190-7.
[30]S. Mouchti, M. R. Whitehouse, A. Sayers, L. P. Hunt, A. J. MacGregor, and A. W. Blom, “The Association of Body Mass Index with Risk of Long-Term Revision and 90-Day Mortality Following Primary Total Hip Replacement: Findings from the National Joint Registry for England, Wales, Northern Ireland and the Isle of Man.,” Journal of Bone and Joint Surgery, American Volume, vol. 100, no. 24, pp. 2140–2152, Dec. 2018, doi: 10.2106/JBJS.18.00120.
[31]J. Chen et al., “Impact of chronic kidney disease on outcomes after total joint arthroplasty: a meta-analysis and systematic review,” International Orthopaedics, vol. 44, no. 2, pp. 215–229, Feb. 2020, doi: 10.1007/S00264-019-04437-4.
[32]A. Bonnefoy-Mazure, D. Dellagiovanna, C. Barea, D. Hannouche, and A. Lübbeke, “Association of preoperative health status with risk of complications after primary total hip arthroplasty: how useful are the measures self-rated health, ASA classification and comorbidity count?,” BMC Musculoskeletal Disorders, vol. 26, July 2025, doi: 10.1186/s12891-025-08745-2.
[33]J. A. Malkani et al., “Complications and Readmission Incidence Following Total Hip Arthroplasty in Patients Who Have End-Stage Renal Failure.,” Journal of Arthroplasty, vol. 35, no. 3, pp. 794–800, Mar. 2020, doi: 10.1016/J.ARTH.2019.10.042.
[34]J. D. Walls, D. Abraham, C. L. Nelson, A. F. Kamath, N. M. Elkassabany, and J. Liu, “Hypoalbuminemia More Than Morbid Obesity Is an Independent Predictor of Complications After Total Hip Arthroplasty,” Journal of Arthroplasty, vol. 30, no. 12, pp. 2290–2295, Dec. 2015, doi: 10.1016/J.ARTH.2015.06.003.
[35]Q. Lian, J. Wang, Y. Lian, Q. Yang, M. Zhao, and Y. Zhang, “Impact of valvular heart disease on hip replacement: a retrospective nationwide inpatient sample database study.,” BMC Musculoskeletal Disorders, vol. 22, no. 1, p. 860, Oct. 2021, doi: 10.1186/S12891-021-04738-Z.
[36]I. E. Ashkenazi, J. Thomas, K. W. Lawrence, M. Meftah, J. C. Rozell, and R. Schwarzkopf, “The Impact of Obesity on Total Hip Arthroplasty Outcomes when Performed by High Volume Surgeons - A Propensity Matched Analysis from a High-Volume Urban Center.,” Journal of Arthroplasty, Feb. 2024, doi: 10.1016/j.arth.2024.02.066.
[37]P. Lan, X. Chen, Z.-S. Fang, J. Zhang, S. Liu, and Y. Liu, “Effects of Comorbidities on Pain and Function After Total Hip Arthroplasty,” Frontiers in Surgery, vol. 9, May 2022, doi: 10.3389/fsurg.2022.829303.
[38]R. J. Ferguson et al., “Does pre-existing morbidity influences risks and benefits of total hip replacement for osteoarthritis: a prospective study of 6682 patients from linked national datasets in England.,” BMJ Open, vol. 11, no. 9, Sept. 2021, doi: 10.1136/BMJOPEN-2020-046712.
[39]S. T. J. Tsang and P. Gaston, “Adverse peri-operative outcomes following elective total hip replacement in diabetes mellitus: A systematic review and meta-analysis of cohort studies,” Journal of Bone and Joint Surgery-british Volume, no. 11, pp. 1474–1479, Nov. 2013, doi: 10.1302/0301-620X.95B11.31716.
[40]A. Postler, C. Lützner, T. Lange, J. Schmitt, J. Lützner, and K.-P. Günther, “[Decision for total hip arthroplasty-the surgeons’ view].,” Orthopade, vol. 50, no. 4, pp. 278–286, Mar. 2021, doi: 10.1007/S00132-021-04078-9.
[41]N. Meißner et al., “Outcomes of total hip arthroplasty in obese patients with and without preoperative weight loss: A systematic review and meta‐analysis,” Journal of Experimental Orthopaedics, vol. 13, Jan. 2026, doi: 10.1002/jeo2.70651.
[42]K. E. Ponnusamy, L. E. Somerville, R. W. McCalden, J. D. Marsh, and E. M. Vasarhelyi, “Revision Rates and Functional Outcome Scores for Severely, Morbidly, and Super-Obese Patients Undergoing Primary Total Hip Arthroplasty: A Systematic Review and Meta-Analysis.,” Jbjs reviews, vol. 7, no. 4, Apr. 2019, doi: 10.2106/JBJS.RVW.18.00118.
[43]Y. Elsiwy, I. A. Jovanovic, K. Doma, K. Hazratwala, and H. L. Letson, “Risk factors associated with cardiac complication after total joint arthroplasty of the hip and knee: a systematic review,” Journal of Orthopaedic Surgery and Research, vol. 14, no. 1, pp. 1–12, Jan. 2019, doi: 10.1186/S13018-018-1058-9.
[44]M. Akhtar, D. I. Razick, R. Kamran, U. Ansari, R. Khalil, and S. Preiss-Farzanegan, “Patient-Reported Outcomes and Factors Impacting Success of the Periacetabular Osteotomy,” Cureus, vol. 15, Apr. 2023, doi: 10.7759/cureus.37320.
[45]Y. Murata et al., “Comparison Between Hip Arthroscopic Surgery and Periacetabular Osteotomy for the Treatment of Patients With Borderline Developmental Dysplasia of the Hip: A Systematic Review:,” Orthopaedic Journal of Sports Medicine, vol. 9, no. 5, pp. 23259671211007401–23259671211007401, May 2021, doi: 10.1177/23259671211007401.
[46]J. C. Clohisy, A. L. Schutz, L. C. S. John, P. L. Schoenecker, and R. W. Wright, “Periacetabular osteotomy: a systematic literature review.,” Clinical Orthopaedics and Related Research, vol. 467, no. 8, pp. 2041–2052, Apr. 2009, doi: 10.1007/S11999-009-0842-6.
[47]P. Lodhia, S. Chandrasekaran, C. Gui, N. Darwish, C. Suarez-Ahedo, and B. G. Domb, “Open and Arthroscopic Treatment of Adult Hip Dysplasia: A Systematic Review,” Arthroscopy, vol. 32, no. 2, pp. 374–383, Feb. 2016, doi: 10.1016/J.ARTHRO.2015.07.022.
[48]T. D. Lerch, S. D. Steppacher, E. F. Liechti, M. Tannast, and K. A. Siebenrock, “One-third of Hips After Periacetabular Osteotomy Survive 30 Years With Good Clinical Results, No Progression of Arthritis, or Conversion to THA.,” Clinical Orthopaedics and Related Research, vol. 475, no. 4, pp. 1154–1168, Apr. 2017, doi: 10.1007/S11999-016-5169-5.
[49]J. Tan, S. H. S. Tan, M. S. Rajoo, A. K. S. Lim, and J. H. P. Hui, “Hip survivorship following the Bernese Periacetabular Osteotomy for the treatment of Acetabular Dysplasia: A Systematic Review and Meta-analysis.,” Orthopaedics & Traumatology-surgery & Research, vol. 108, no. 4, pp. 103283–103283, Apr. 2022, doi: 10.1016/j.otsr.2022.103283.
[50]J. C. Clohisy, A. L. Schutz, P. L. Schoenecker, and R. W. Wright, “A Systematic Literature Review,” Jan. 2009.
[51]A. Kaneuji, T. Sugimori, T. Ichiseki, K. Fukui, E. J. Takahashi, and T. Matsumoto, “Rotational Acetabular Osteotomy for Osteoarthritis with Acetabular Dysplasia: Conversion Rate to Total Hip Arthroplasty within Twenty Years and Osteoarthritis Progression After a Minimum of Twenty Years.,” Journal of Bone and Joint Surgery, American Volume, vol. 97, no. 9, pp. 726–732, May 2015, doi: 10.2106/JBJS.N.00667.
[52]S. N. Sambandam, J. R. Hull, and W. A. Jiranek, “Factors predicting the failure of Bernese periacetabular osteotomy: a meta-regression analysis.,” International Orthopaedics, vol. 33, no. 6, pp. 1483–1488, Dec. 2009, doi: 10.1007/S00264-008-0643-7.
[53]P. England and R. S. Selley, “Indications for Acetabular and Femoral Osteotomies for the Non-Arthritic Hip,” Current Reviews in Musculoskeletal Medicine, vol. 19, no. 1, pp. 3–3, Oct. 2025, doi: 10.1007/s12178-025-09996-1.
[54]V. J. Leopold, C. Hipfl, C. Perka, S. Hardt, and L. Becker, “Periacetabular osteotomy for symptomatic hip dysplasia in middle aged patients: does age alone matter?,” Archives of Orthopaedic and Trauma Surgery, Dec. 2023, doi: 10.1007/s00402-023-05160-x.
[55]Y. Yasunaga, S. Oshima, T. Shoji, N. Adachi, and M. Ochi, “A 30-year follow-up study of rotational acetabular osteotomy for pre- and early-stage osteoarthritis secondary to dysplasia of the hip,” Bone and Joint, vol. 106-B, no. 5 Supple B, pp. 25–31, May 2024, doi: 10.1302/0301-620x.106b5.bjj-2023-0818.r1.
[56]E. N. Novais, S. L. Ferraro, P. E. Miller, Y.-J. Kim, M. B. Millis, and J. C. Clohisy, “Periacetabular Osteotomy for Symptomatic Acetabular Dysplasia in Patients ≥40 Years Old: Intermediate and Long-Term Outcomes and Predictors of Failure.,” Journal of Bone and Joint Surgery, American Volume, May 2023, doi: 10.2106/JBJS.23.00001.
[57]A. T. Rif’ah, “Risk Factors for Composite Failure of Hip Dysplasia Treated With Periacetabular Osteotomy: A Minimum 10-Year Follow-up,” Journal of the American Academy of Orthopaedic Surgeons, vol. 30, no. 8, pp. e690–e702, Feb. 2022, doi: 10.5435/jaaos-d-21-00535.
[58]N. Ziran et al., “Ten- and 20-year Survivorship of the Hip After Periacetabular Osteotomy for Acetabular Dysplasia.,” Journal of The American Academy of Orthopaedic Surgeons, vol. 27, no. 7, pp. 247–255, Apr. 2019, doi: 10.5435/JAAOS-D-17-00810.
[59]T. Yuasa, K. Maezawa, K. Kaneko, and M. Nozawa, “Rotational acetabular osteotomy for acetabular dysplasia and osteoarthritis: a mean follow-up of 20 years,” Archives of Orthopaedic and Trauma Surgery, vol. 137, no. 4, pp. 465–469, Feb. 2017, doi: 10.1007/S00402-017-2636-8.
[60]Y. Yasunaga, M. Ochi, T. Yamasaki, T. Shoji, and S. Izumi, “Rotational Acetabular Osteotomy for Pre- and Early Osteoarthritis Secondary to Dysplasia Provides Durable Results at 20 Years,” Clinical Orthopaedics and Related Research, vol. 474, no. 10, pp. 2145–2153, Apr. 2016, doi: 10.1007/S11999-016-4854-8.
[61]L. Pichler, S. Ahmad, L. Pichler, and S. Ahmad, “Rising star editorial: Periacetabular osteotomy—Reliable outcome and expanding indications,” Journal of Experimental Orthopaedics, vol. 12, no. 4, pp. e70499–e70499, Oct. 2025, doi: 10.1002/jeo2.70499.
[62]M. Tomioka et al., “Ten-year survival rate after rotational acetabular osteotomy in adulthood hip dysplasia,” BMC Musculoskeletal Disorders, vol. 18, no. 1, pp. 191–191, May 2017, doi: 10.1186/S12891-017-1556-7.
[63]Y. Yasunaga, S. Ohshima, T. Shoji, and N. Adachi, “Thirty-year follow-up study of rotational acetabular osteotomy,” Orthopaedic proceedings/Journal of bone and joint surgery. British volume. Orthopaedic proceedings, vol. 105-B, no. SUPP_12, pp. 60–60, June 2023, doi: 10.1302/1358-992x.2023.12.060.
[64]S. S. Ahmad, M. Haertlé, C. Konrads, A. Derksen, H. Windhagen, and N. Wirries, “The Scientific Evolution of Periacetabular Osteotomy: A Global Review,” Stomatology, vol. 11, no. 20, pp. 6099–6099, Oct. 2022, doi: 10.3390/jcm11206099.
[65]T. D. Lerch, S. D. Steppacher, E. F. Liechti, K. A. Siebenrock, and M. Tannast, “Periazetabuläre Osteotomie nach Ganz,” Orthopade, vol. 45, no. 8, pp. 687–694, June 2016, doi: 10.1007/S00132-016-3265-6.
[66]S. Hamai et al., “Minimum 10-Year Clinical Outcomes After Periacetabular Osteotomy for Advanced Osteoarthritis Due to Hip Dysplasia,” Orthopedics, vol. 41, no. 5, pp. 300–305, Sept. 2018, doi: 10.3928/01477447-20180806-04.
[67]N. Ramadanov et al., “Conservative treatment versus hip arthroscopy in patients with femoroacetabular impingement,” Bone & joint open, vol. 6, no. 4, pp. 480–498, Apr. 2025, doi: 10.1302/2633-1462.64.bjo-2024-0198.r1.
[68]S. S. Mahmoud, A. Takla, D. Meyer, D. R. Griffin, and J. O’Donnell, “Arthroscopic hip surgery offers better early patient-reported outcome measures than targeted physiotherapy programs for the treatment of femoroacetabular impingement syndrome: a systematic review and meta-analysis of randomized controlled trials,” Journal of Hip Preservation Surgery, vol. 9, no. 2, pp. 107–118, Mar. 2022, doi: 10.1093/jhps/hnac012.
[69]D. N. W. Kim et al., “Short Symptom Duration is Associated With Superior Outcomes in Patients Undergoing Primary Hip Arthroscopy: A Systematic Review.,” Arthroscopy, vol. 39, no. 2, pp. 498–509, Nov. 2022, doi: 10.1016/j.arthro.2022.11.009.
[70]D. de Sa et al., “A Systematic Summary of Systematic Reviews on the Topic of Hip Arthroscopic Surgery,” Orthopaedic Journal of Sports Medicine, vol. 6, no. 9, pp. 2325967118796222–2325967118796222, Sept. 2018, doi: 10.1177/2325967118796222.
[71]M. Hassan et al., “Open and arthroscopic management of femoroacetabular impingement: a review of current concepts,” Journal of Hip Preservation Surgery, vol. 9, no. 4, pp. 265–275, Oct. 2022, doi: 10.1093/jhps/hnac043.
[72]M. Sansone et al., “Outcome of hip arthroscopy in patients with mild to moderate osteoarthritis—A prospective study,” Journal of Hip Preservation Surgery, vol. 3, no. 1, pp. 61–67, Apr. 2016, doi: 10.1093/JHPS/HNV079.
[73]S. Daivajna, A. A. Bajwa, and R. N. Villar, “Outcome of arthroscopy in patients with advanced osteoarthritis of the hip.,” PLOS ONE, vol. 10, no. 1, Jan. 2015, doi: 10.1371/JOURNAL.PONE.0113970.
[74]B. G. Domb, C. Gui, and P. Lodhia, “How Much Arthritis Is Too Much for Hip Arthroscopy: A Systematic Review,” Arthroscopy, vol. 31, no. 3, pp. 520–529, Mar. 2015, doi: 10.1016/J.ARTHRO.2014.11.008.
[75]D. Parry, J. Dhillon, G. Embree, and M. Kraeutler, “EP195 There is Evidence that Hip Arthroscopy for Femoroacetabular Impingement Reduces the Risk for Developing Hip Osteoarthritis: A Systematic Review,” Journal of Hip Preservation Surgery, vol. 12, pp. ii99–ii99, Dec. 2025, doi: 10.1093/jhps/hnaf069.317.
[76]O’Connor, Ince, Clohisy, and Willey, “Hip Dysplasia Treated With Periacetabular Osteotomy in Patients Over 40 Years Old: A Systematic Review.,” The Iowa orthopaedic journal, 2024, [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/38919352
[77]Wilson, Wagner, and Spiker, “Borderline Hip Dysplasia - Best Treated with Hip Arthroscopy or Periacetabular Osteotomy?,” Current reviews in musculoskeletal medicine, 2024, doi: 10.1007/s12178-024-09928-5.
[78]H. Robert, P. Robert, D. Dobromir, and B. Roland, “Periacetabular osteotomy versus hip arthroscopy in patients with borderline developmental dysplasia of the hip: A systematic review and multi‐level meta‐analysis,” Nov. 2025, doi: 10.82491/opusthd-39.
[79]C.-H. Kim and J. W. Kim, “Periacetabular osteotomy vs. total hip arthroplasty in young active patients with dysplastic hip: Systematic review and meta-analysis.,” Orthopaedics & Traumatology-surgery & Research, vol. 106, no. 8, pp. 1545–1551, Dec. 2020, doi: 10.1016/J.OTSR.2020.08.012.
[80]Ferguson, Palmer, Taylor, Porter, Malchau, and Glyn-Jones, “Hip replacement.,” Lancet (London, England), 2018, doi: 10.1016/S0140-6736(18)31777-X.
[81]J. K. Tse, “Total Hip Arthroplasty: Indications and Contraindications,” pp. 3–7, Jan. 2022, doi: 10.1007/978-981-19-3606-7_1.
[82]“Decision Making in Borderline Cases between Hip Preservation and Reconstruction Surgery,” Nov. 2022, doi: 10.5772/intechopen.104765.
[83]S. Rahm and P. O. Zingg, “Indikationen zum Gelenkersatz : Hüfttotalendoprothese,” Zeitschrift Fur Rheumatologie, vol. 77, no. 1, pp. 55–65, Feb. 2018, doi: 10.1007/S00393-017-0408-Z.
[84]F. Luceri et al., “Medium-term outcomes of total hip arthroplasty in juvenile patients,” Journal of Orthopaedic Surgery and Research, vol. 15, no. 1, pp. 1–7, Oct. 2020, doi: 10.1186/S13018-020-01990-2.
ごあいさつ

長引いた痛みを一人で治すのは困難なことが多いです。
困ったときは自身で判断せずに適切な処置を受けるために専門家に相談しましょう。
もし、お近くにお住まいで、困っているならば、一度ひまわり接骨院までお問い合わせください。腰痛・坐骨神経痛の専門家の新幡が、ご相談に乗ります。
気軽にご相談ください。

新着情報・お知らせ
お気軽にお問合せください

お電話でのお問合せ・相談予約
<受付時間>
月~土
9:00〜13:00 /15:00〜19:00
※日曜・祝日は除く
フォームは24時間受付中です。お気軽にご連絡ください。
ひまわり接骨院

住所
〒213-0002
神奈川県川崎市高津区二子1丁目7−17 リバーサイドマンション杉崎 102
アクセス
二子新地駅 徒歩3分
駐車場:近隣にコインパーキングあり。自転車・バイクは店舗前に駐輪場がございます。
受付時間
月~土
9:00〜13:00 /15:00〜19:00
定休日
日曜・祝日

