
〒213-0002 神奈川県川崎市高津区二子1丁目7−17
リバーサイドマンション杉崎 102 二子新地駅 徒歩3分
| 月 | 火 | 水 | 木 | 金 | 土 | 日祝 | |
|---|---|---|---|---|---|---|---|
| 9:00〜13:00 | ● | ● | ● | ● | ● | ● | ─ |
| 15:00〜19:00 | ● | ● | ● | ● | ● | ● | ─ |
変性腰椎すべり症の重症度を決めるのは?
公開日:2026/06/29
更新日:2026/00/00
このレポートは、変性腰椎すべり症(DLS)の重症度や予後を予測する要因について、2016年以降の科学的根拠に基づき包括的に解説しています。
骨盤入射角(PI)や矢状面垂直軸(SVA)といった生体力学的パラメータに加え、椎間板の状態や多裂筋の萎縮などの画像所見が、病状の進行や治療の成否に深く関与していることを示しています。
また、運動恐怖やうつ症状などの心理社会的因子が術後の生活の質に与える影響を強調し、身体的側面のみならず多角的な評価が必要であると説いています。
さらに、機械学習を用いた患者の層別化や、除圧術に固定術を追加する妥当性についても最新のエビデンスを提供しています。
結論として、これらの多様な因子を統合的に判断することで、患者一人ひとりに最適化された個別化医療の実現と、共有意思決定の促進が可能になると結論付けています。
目次
変性腰椎すべり症(DLS)の重症度や予後を予測する主要な知見は、生体力学的パラメータ、画像所見、心理社会的因子などの多面的な評価によって構成されています。
各カテゴリーの主要な予測因子は以下の通りです。
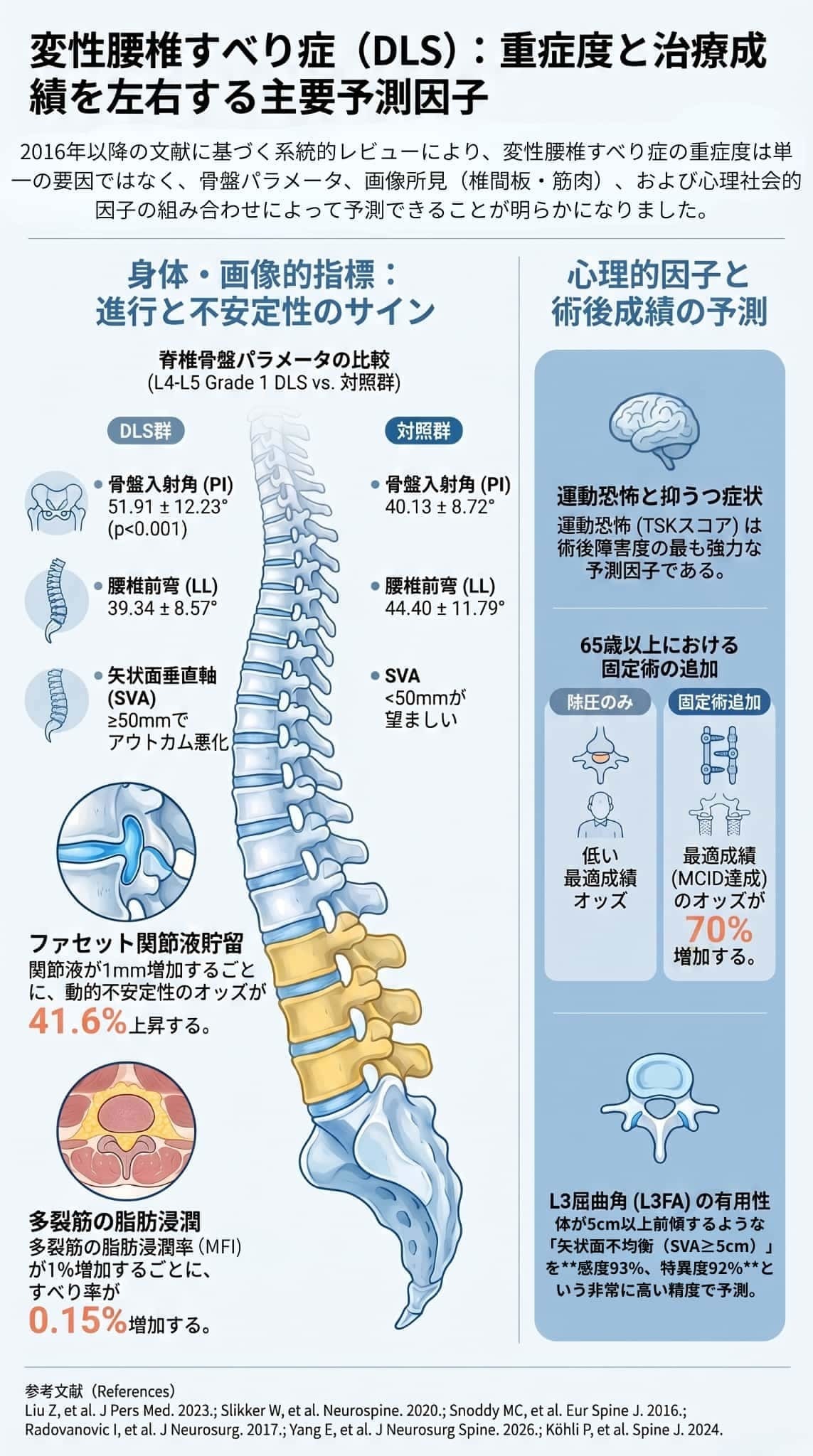
- 骨盤傾斜角(PI): PIは単一レベルグレード1の変性腰椎すべり症(DLS)発症の重要な予測因子であり、変性腰椎すべり症(DLS)患者では対照群と比較して有意に高値を示します。
- 腰椎前弯(LL): DLS患者では腰椎前弯が対照群に比べて有意に低下していることが確認されています。
- 矢状面垂直軸(SVA): SVAは全身のバランスや患者報告アウトカム(ODIや腰痛など)の重要な予測因子です。術後のSVAが50mm以上の場合、身体的機能や痛みのスコアが有意に悪化することが示されています。
- L3屈曲角(L3FA): 多椎間変性腰椎すべり症(DLS)において、L3FAの増加は矢状面不均衡(SVA≥5cm)を高精度で予測し、保存療法の失敗や機能障害の悪化と関連する新しいパラメータです。
・用語解説
※骨盤傾斜角(PI):骨盤の仙骨(背骨の土台)の傾きと、股関節(大腿骨頭)の位置関係からレントゲン画像を用いて算出されます。
※腰椎前弯(LL):腰の骨(腰椎)が前方に向かってゆるやかにカーブしている生理的な弯曲構造のこと
※矢状面垂直軸(SVA):体を横(矢状面)から見たときに、頭部から重心がどれくらい前方に傾いているかを示す指標。測定方法: 第7頸椎(首の付け根)の中心から下ろした垂直線と、仙骨(骨盤の後方にある骨)の後上縁との間の水平距離で測ります。
※L3曲げ角度(L3FA)は、通常、X線撮影で測定される矢状面における3番目の腰椎(L3)の屈曲を評価するために使用される新しい腰部パラメータです。このパラメータは、脊椎の生体力学とその位置合わせの理解に役立つ、より広範な脊椎骨盤測定値の一部です。
- 椎間板高の保持: 椎間板の高さが保たれていることは、動的不安定性と有意に関連しており、将来的なすべり進行の可能性を示唆します。
- ファセット関節液貯留: ファセット関節液は動的不安定性の重要な指標です。関節液が1mm増加するごとに動的不安定性のリスクが41.6%増加するとされています。
- 多裂筋(Multifidus)の萎縮と脂肪浸潤: 多裂筋の機能的断面積の減少や脂肪浸潤の増加は、すべり率の増加や疾患の進行リスクと有意に相関し、重症度の指標となります。
- 椎間板内真空現象(IVP): IVPの重症度が増加すると、腰痛の悪化やODIスコアの低下と関連し、固定術の適応が増加する傾向があります。
- うつ症状と不安: うつ症状は術前障害度の重要な予測因子であり、術後早期の回復遅延や満足度の低下とも関連しています。不安もODI改善と負の相関を示し、術後満足度に影響します。
- 運動恐怖(Kinesiophobia): 「動かすと悪化する」という運動恐怖は、術後障害度の最も強力な予測因子のひとつとされています。
- 術前の症状強度: 術前の腰痛スコアが低い患者の方が最適な術後成績を得られやすい一方で、重度の障害を持つ患者は、術後の絶対的なスコアは劣るものの、改善の幅(実感)は大きいという特徴があります。
現状において、変性腰椎すべり症(DLS)の発症や進行に関連する特異的な遺伝的・生物学的バイオマーカーは確立されていません。一般的な腰椎椎間板変性の遺伝性や、炎症性バイオマーカーに関する研究は進んでいますが、変性腰椎すべり症(DLS)特化の臨床予測因子としては今後の研究課題とされています。
変性腰椎すべり症(DLS)の重症度予測や治療方針の決定においては、これらの因子を単独で評価するのではなく、複合的・統合的に評価することが不可欠です。
例えば、画像所見で動的不安定性が見られ、SVAが高く心理的なうつ傾向を伴う患者に対しては、それらを総合して保存療法の限界を見極めたり、手術術式(除圧単独か固定術の追加か)を選択するなど、個別化医療の実現に向けた活用が推奨されています。
変性腰椎すべり症(DLS)の重症度や予後予測において極めて重要な「生体力学的・脊椎骨盤パラメータ」の具体的な知見について、以下の通り解説します。
骨盤入射角(PI)は、変性腰椎すべり症(DLS)の発症を予測する上で非常に重要な因子です。
- 成人における発症の強力な予測因子: 単一レベル(L4-L5)のグレード1 変性腰椎すべり症(DLS)患者のPIは平均51.91±12.23°であり、対照群(40.13±8.72°)と比較して有意に高いことが示されています。女性変性腰椎すべり症(DLS)患者に特化した研究でも、PIは椎体高比とともに変性腰椎すべり症(DLS)発症の独立した予測因子とされています。
- 小児(成長期)における特例: 一方で、小児の低グレードすべり症では、追跡期間中にPIの有意な増加が見られたものの、それがすべり率や腰仙角の進行(悪化)とは関連していないことが示されており、成人の変性腰椎すべり症(DLS)とは異なる点に注意が必要です。
- DLS特有の低下: 変性腰椎すべり症(DLS)患者のLLは平均39.34±8.57°と、対照群(44.40±11.79°)より有意に低下しています。これは、逆にLLが高値を示すIsthmic型(分離)すべり症とは対照的な特徴です。
- 局所冠状面不均衡(LCI)との関連: LCIを伴う変性腰椎すべり症(DLS)患者では、LLの低下がさらに顕著(平均38.3°)になります。
- 術後アウトカムへの影響: 術前にLLが35度以上保たれている患者は、歩行障害の改善率が高いことが報告されています。また、術後のLLの過少(PIとのミスマッチなど)は、後述するSVAの悪化と関連しています。
- アウトカム悪化の独立した危険因子: 術後のSVAが50mm以上の場合、SF-36(身体的QOLスコア)、ODI(機能障害スコア)、腰痛VAS(痛みのスコア)が有意に悪化します。SVAの増加はODI悪化の独立した危険因子でもあります。また、SVAの増加はSF-36身体的サマリースコアと負の相関、ODIと正の相関を示します。
- 保存療法との関連: 高いSVAは、保存療法が失敗する予測因子となる可能性が示唆されています。
- すべり症患者のPTは21.30±7.42°と、対照群(13.03±7.72°)より有意に高値を示します。
- PT自体は保存療法の成績や進行とは直接関連しないとされていますが、術後3ヶ月の早期において、PTが高いことは症状改善(MCID:最小臨床的重要差)を達成できない予測因子となることが報告されています。
- L3FAは、多椎間DLSにおいて術前の矢状面不均衡(SVAが5cm以上となる状態)を非常に高い精度(感度93%、特異度92%)で予測します。
- L3FAの増加は、患者の機能障害(ODI悪化)や保存療法の失敗率上昇と有意に関連しており、手術適応(特に保存療法の限界)を判断する上で重要な指標となります。
これらの生体力学的・脊椎骨盤パラメータは、変性腰椎すべり症(DLS)の発症リスクを評価するだけでなく、「保存療法で効果が期待できるか」「固定術などの手術を追加すべきか」「術後の患者の生活の質(QOL)はどう変化するか」といった治療戦略を決定する上で、非常に重要な客観的指標となります。
変性腰椎すべり症(DLS)の重症度や進行、そして「動的不安定性」を予測する上で、解剖学的・画像所見は極めて重要な役割を果たします。
最新の研究に基づく具体的な指標とエビデンスについて、以下の通り詳しく解説します。
椎間板の状態は、変性腰椎すべり症(DLS)の発症と進行の双方に深く関わっています。
- 椎間板変性(DD): 椎間板の変性度合い(Pfirrmann分類などで評価)は、すべり症進行の独立した危険因子のひとつです。
- 椎間板高の保持: 興味深いことに、椎間板の高さが「保たれている」ことは、逆に動的不安定性の強力な予測因子となります。椎間板の高さが残っていると椎体間が動きやすくなり、将来的なすべり進行の可能性が高まることが示唆されています。
背中側にあるファセット関節の状態は、重症度と動的不安定性を評価する中心的な要素です。
- ファセット関節の角度と形態: ファセット関節角(FJA)が矢状面方向(縦方向)に向いているほど、あるいは骨関節症が重度であるほど、疾患進行の独立した危険因子となります。
- ファセット関節液の貯留: 関節内に水が溜まる(関節液貯留)ことは、動的不安定性の最も重要な指標の一つです。ファセット関節液が1mm増加するごとに、動的不安定性のオッズ(リスク)が41.6%増加し、逆に関節液が0.5mm未満であれば動的不安定性がない確率が90%に達すると報告されています。
腰椎を支える深層の筋肉である多裂筋の変性も、すべりの重症度と直接相関します。
- 脂肪への置き換わり(脂肪浸潤): 多裂筋の機能的断面積の減少(萎縮)や、筋肉が脂肪に置き換わる「脂肪浸潤率(FIA%)」の増加は、すべり率の増加と正の相関を示します。
- 進行の危険因子: 多裂筋の脂肪浸潤率は、変性腰椎すべり症(DLS)疾患進行の独立した危険因子として同定されており、予測モデルにも組み込まれています。
- 椎間板内真空現象(IVP): 椎間板内にガスが溜まる現象(IVP)の重症度が増すにつれて、腰痛のオッズ比やODI(機能障害スコア)悪化のオッズ比が約1.7〜1.9倍に高まることが示されています。また、IVPの重症度は固定術が適応される可能性の増加とも関連しています。
- 椎間孔狭窄: 変性腰椎すべり症(DLS)に脊柱管狭窄症を伴う場合、感覚や運動の障害が有意に出現しやすく、症状の重症度と統計学的に有意な関連を示します。
- 座位での撮影: 座った状態(自然座位)でのX線撮影は、通常の立ち上がり時よりも高い滑脱率(すべりの程度)や後弯角を示すことがあり、動的不安定性の検出に非常に有用であるとされています。
- MRIによる不安定性指標(MRIPs): MRI画像から不安定性を推測する指標として、「両側ファセット関節角が46度以上」「両側ファセット関節液が1.5mm以上」「椎間板高指数が13%以上」という基準が提案されており、これらを満たす場合はX線画像で明らかなすべりがなくても不安定性が潜んでいる可能性が高いとされています。
変性腰椎すべり症(DLS)における心理社会的因子は、身体的・画像的因子と同等かそれ以上に、術前の障害度や術後成績を予測する上で極めて重要な役割を果たします。
具体的な予測因子として、以下の要素が最新の研究で示されています。
- 術前の運動恐怖スコア(TSK)は、術後1年以上経過した時点での障害度と有意に関連することが示されています。
- 痛みによる身体的な制限だけでなく、下肢機能を要する日常生活動作(ADL)や社会参加においても、うつ症状と並んで最も強力な予測因子として機能します。
- 術前障害度の予測: 痛みの強度や年齢、性別(女性)とともに、うつ症状の有無は術前の障害度を有意に予測します。
- 早期回復への影響: うつ症状がある患者は、術後早期(3ヶ月時点)における改善が遅れる予測因子となります(ただし、6ヶ月以降ではその関連は有意性を失うとされています)。
- 満足度と再手術: 術後もうつ症状が持続すると、機能改善率が低下し手術満足度も下がります。さらに、抗うつ薬の使用は再手術リスクを約2倍(ハザード比2.08)に高める危険因子として報告されています。
- 術前の不安スコアが高いと、術後の機能障害(ODI)の改善が乏しくなる傾向(負の相関)があります。
- うつと同様に、術後も不安症状が持続する患者は機能改善率や手術満足度が有意に低いことが示されています。
- 改善幅と絶対値の乖離: 術前の機能障害(ODIスコアなど)が非常に重度な患者は、術後の絶対的なスコアは軽症患者より劣る傾向がありますが、「改善の幅(実感)」は軽症患者よりも有意に大きく、最小臨床的重要差(MCID)の達成率も高いという特徴があります。一方で、ベースラインの疾患負荷が高い患者群は術後満足度が低い傾向もみられます。
※疾病負荷(Disease Burden)とは、ある集団における病気やケガによる健康への悪影響を、死亡率や罹患率、生活の質(QOL)の低下、経済的コストなどを総合的に考慮して数値化した指標です。
- 精神衛生の良好さ: 術前の精神衛生状態(SF-36 MCSスコアなど)が良好であることが、術後の十分な機能改善、高い満足度、そして「期待の充足」を強力に予測します。また、術前の腰痛スコアが比較的低い(痛みが強すぎない)状態のほうが、結果として最適な術後成績を得やすいとされています。
変性腰椎すべり症(DLS)の重症度や進行予測に関する遺伝的・生物学的因子とバイオマーカーについては、現状ではまだ研究の途上にある領域です。ソースから得られる主要な知見を以下にまとめます。
最も重要な点として、現時点(提供された2016年以降の文献に基づく)において、変性腰椎すべり症(DLS)の発症や重症度に特化した、臨床予測因子として確立されている特異的な遺伝的・生物学的バイオマーカーは存在していません。現在利用されている指標は、主に腰椎疾患全般に関する知見からの推測にとどまっています。
- 構造・コラーゲン関連遺伝子: COL1A1、COL9A2、ACANなどの多型は、椎間板ヘルニアのリスク増加と関連しています。
- 炎症性・異化関連遺伝子: IL1A、IL1B、IL6などの炎症性サイトカイン関連遺伝子や、MMP3などの異化遺伝子は、椎間板変性やModic変化(骨髄の変性)のリスク増加と関連しています。
- 疼痛調節遺伝子: COMTやOPRM1といった遺伝子の多型は、患者が感じる疼痛の強さに関連しているとされています。
- リスクを増加させるもの: STAMBP(STAM結合タンパク質)やCD6アイソフォーム。
- リスクを低下させるもの: MCP2(単球走化性タンパク質2)やLAP-TGF-β1。 これらの知見は脊椎変性疾患全般に関するものですが、将来的なバイオマーカー候補としての可能性を示しています。
固定術などの手術を受けた後、手術部位の隣の椎間板が変性してしまう「隣接椎間板変性(ASDD)」に対して、年齢とともに遺伝的因子が大きく影響することがわかっています。
例えば、炎症性遺伝子であるIL18RAPの多型は隣接レベルの椎間板高低下(悪化)と関連し、逆にMMP-9遺伝子の多型は椎間板高の維持と関連していることが報告されています。
生体力学的パラメータや画像所見がすでに強力な予測因子として機能している一方で、遺伝的・生物学的因子は「患者個人がなぜ重症化しやすいのか」を根底から説明するための重要なピースです。
今後、変性腰椎すべり症(DLS)患者を対象とした大規模な遺伝的関連研究が進み、炎症性バイオマーカーなどを組み合わせた予測モデルが構築されることで、より精度の高い**個別化医療(精密医療)**が実現することが期待されています。
変性腰椎すべり症(DLS)の重症度や術後成績を評価する上で、患者自身が主観的な痛みや生活の質を評価する「患者報告アウトカム(PRO)」は極めて重要です。
参考文献に基づく主要な知見を以下にまとめます。
- 術前の痛みの強さ: 術前の腰痛スコア(NRSなど)が比較的低い(痛みが強すぎない)患者の方が、最適な術後成績を得られやすい傾向があります。
- 改善幅との関連: 一方で、術前の症状(VASやODI)が重度な患者ほど、術後における腰痛の改善幅は大きくなり、治療によって意味のある改善(最小臨床的重要差:MCID)を達成する割合が高くなることが分かっています。
- 精神衛生と社会的背景: 術前の精神衛生状態(SF-36のMCSスコアなど)が良好であることが、ODIのMCID達成の重要な予測因子となります。また、術前に就労していることもODIの改善と有意に関連しています。
- 生体力学的・画像的要因との関連: L3屈曲角(L3FA)の増加や多裂筋の変性といった身体的な悪化所見は、術後のODI悪化(機能障害の残存)と関連しています。また、固定術を追加することがODIの改善に関連するという報告もあります。
- 矢状面バランス(SVA)の影響: 体の前傾を示す矢状面垂直軸(SVA)が50mm以上になると、SF-36の身体的サマリースコア(PCS)が有意に悪化し、SVAの増加は生活の質と負の相関を示します。
- EQ-5D改善の予測因子: 高齢であること、高学歴であること、術前の下肢痛スコアが高いこと、そして術前のQOLが良好であることが、EQ-5D(全般的なQOL指標)改善の予測因子とされています。
術前重症度は、術後の「絶対的なスコア」と「改善幅」の両方に影響を与えます。
- 術前の機能障害が非常に重度(ODIが41以上など)な患者は、術後の痛みスコアや入院期間などの絶対値は軽度患者より劣る傾向があります。
- しかし、術後6週や最終追跡時において、うつ症状(PHQ-9)、腰痛(VAS)、機能障害(ODI)の平均改善幅は重度障害群の方が有意に大きく、MCIDの達成率も高くなります。つまり、術前が重症であるほど、患者が実感する「良くなった度合い」は大きいと言えます。
患者報告アウトカムは、単一の要因ではなく様々な因子と関連しています。
- 生体力学的因子: SVAの増加や全体的冠状面不均衡(GCI)、年齢の増加がODI悪化の独立した危険因子となります。不安定性や局所冠状面不均衡(LCI)は、腰痛や下肢痛の増加と関連します。
- 画像所見: 椎間板高、ファセット関節角、側方すべりなどの画像所見も、術後早期や長期の臨床成績(PRO)と関連することが機械学習を用いた研究で示されています。
このように、患者報告アウトカムを最大化・適正化するためには、画像所見や生体力学的なバランスだけでなく、術前の痛みの程度や精神衛生状態、就労状況などの心理社会的因子も考慮した上で、患者の期待値を適切に管理することが重要とされています。
変性腰椎すべり症(DLS)の治療において、保存療法で効果が得られるか、あるいは手術(除圧単独か、固定術を追加するか)を選択すべきかを予測・判断するための因子については、近年多くのエビデンスが蓄積されています。
主要な予測因子と治療選択の基準は以下の通りです。
生体力学的なバランスの崩れや動的な不安定性が強い場合、保存療法の限界を示す重要なサインとなります。
- L3屈曲角(L3FA)と矢状面不均衡: 多椎間にわたるDLS患者において、L3屈曲角の増加や、高いSVA(矢状面垂直軸:体が5cm以上前傾している状態)は、保存療法の失敗率上昇や機能障害(ODI)の悪化と有意に関連しています。
- 動的不安定性の所見: 画像上での「椎間板高の保持」や「ファセット関節液の貯留(1mm増加ごとに動的不安定性のオッズが41.6%増加)」は動的不安定性の指標であり、保存療法が難航する可能性を示唆します。これらの所見がある場合、早期に手術を検討することでより良好な成績が得られる可能性があります。
- 意思決定スコアの活用: 「すべりの程度」「ファセット関節の離開と関節液貯留」「矢状面不均衡」「腰痛の重症度」の4つが、術式決定において最も重要な因子として同定されています。これらに基づくスコアリングシステム(3点以上で固定術を示唆)は、約80.6%の精度で適切な術式を予測できると報告されています。
年齢と術式選択に関するデータは、機械学習などを用いた解析で興味深い結果を示しています。
- 65歳以上での成績向上: 65歳以上のグレードI DLS患者を対象とした大規模解析では、固定術を追加することが「最適な術後成績(痛みと生活の質の大幅な改善)」の独立した予測因子(オッズ比1.70)であることが判明しました。固定術を受けた患者は、最適成績を達成する確率が70%増加するとされています。
- 年齢のカットオフは存在しない: ただし、成績が良かった群と悪かった群で年齢そのものに有意差はなく、手術適応における明確な年齢のカットオフ(何歳以上ならこの術式、など)は存在しないことが示唆されています。
術式の選択は、アウトカムの向上と周術期リスクのバランス(トレードオフ)によって決まります。
- 固定術のメリットとデメリット: 固定術の追加は、機能障害(ODI)や痛みの改善、患者満足度において優れているという報告(複数のメタアナリシスなど)が多い一方で、手術時間の延長、出血量の増加、入院期間の延長、合併症率の上昇といった明確な周術期負担の増加を伴います。
- 除圧単独の評価: 除圧単独は負担が軽く、一部のメタアナリシスでは腰痛改善や長期成績において固定術に劣らない(非劣性)という結果も出ており、十分な効果が得られる患者も多いとされています。
- 再手術の予測因子: 再手術の一般的な危険因子としては、抗うつ薬の使用(ハザード比2.08)、初診時に神経性跛行がないこと、そして若年であることが挙げられています。なお、術式(除圧単独か固定術か)による再手術率の違いについては、有意差はないとする報告と、差があるとする報告が混在しており、さらなる長期データの蓄積が必要とされています。
変性腰椎すべり症(DLS)の治療を成功に導くためには、「画像上のすべり度」だけで判断するのではなく、矢状面のバランス(SVAやL3FA)、椎間関節の状態(関節液貯留)、患者の年齢や腰痛の重症度を総合的に評価することが重要です。
特に高齢者においては固定術のメリットが大きい可能性がありますが、手術の負担や患者個人のライフスタイルへの希望を考慮した個別化医療・共有意思決定が不可欠です。
変性腰椎すべり症(DLS)の複雑な重症度予測因子を、患者が理解し納得できる実践的なメッセージに変換することは、患者の期待値管理と「共有意思決定(Shared Decision Making)」において非常に重要です。具体的な教育的アプローチとメッセージの変換方法は以下の通りです。
- 実践的メッセージ: 「MRIやレントゲンは背骨の構造を示すものですが、実際の痛みや生活のしづらさは、背骨と骨盤のバランス、筋肉の状態、そして心理的な要因などが複雑に絡み合って決まります」と説明します。
- 具体例: 「同じくらい骨がすべっていても、体全体のバランスが保たれている方は症状が軽く、バランスが崩れている方は症状が重くなることがあります」と伝えます。
- 骨盤入射角(PI): 「骨盤の形を示す生まれつきの角度です。この角度が大きい人は、腰のカーブも大きくする必要があるため、すべり症になるリスクが少し高くなります」。
- 腰椎前弯(LL)と矢状面垂直軸(SVA): 「腰の適切な前カーブ(LL)が保たれていると体重がうまく分散されます。逆に、体が前傾姿勢(SVAが大きい状態)になると、腰や背中の筋肉に常に負担がかかり、痛みや疲れの原因になります」。
- 動的不安定性: 「体を曲げ伸ばしした時に、腰の骨がグラグラと過剰に動いてしまう状態です。これは骨を支える椎間板や靭帯の力が弱まっているサインで、手術で金属などで固定する必要があるかを判断する重要な目安になります」。
- 多裂筋の萎縮: 「腰の骨を奥深くで支えている筋肉が細くなり、脂肪に置き換わっている状態です。この筋肉の元気さが、今後の進行や術後の回復に影響します」。
痛みへの恐怖(運動恐怖)や気分の落ち込みが回復を遅らせることを伝える際は、患者の性格や意志のせいにしないことが重要です。
- 実践的メッセージ: 「『動かすと痛いから怖い』という不安や気分の落ち込みは、手術後の回復スピードや満足度に影響することが研究で分かっています。これはあなたの意志が弱いからではなく、痛みと心の状態が相互に影響し合うためです」と説明します。
- 解決策の提示: 「適切な指導のもとで少しずつ体を動かしていくことで、『動いても大丈夫だ』という自信を取り戻し、回復を早めることができます」と励まし、術前の前向きな気持ち(楽観性)が術後の満足度につながることを伝えます。
手術で「完全に痛みがゼロになる」という非現実的な期待を持たせないよう、正確なデータに基づき説明します。
- 改善幅と限界の理解: 「術前に症状が非常に重かった方は、手術によって『良くなった』という実感(改善幅)はとても大きくなりますが、最終的な痛みの点数としては、元々軽症だった方よりも少し症状が残りやすい傾向があります」と伝えます。
- 現実的な目標設定: 「手術の現実的な目標は、痛みを完全になくすことではなく、日常生活に支障がないレベルまで症状を軽くすることです」と説明します。
- 早期手術の提案: 動的不安定性や強い体の前傾(高いSVA)がある場合は、「お薬やリハビリなどの保存療法の効果が出にくい状態の可能性が高いため、早めに手術を検討した方が良い結果につながりやすいです」と客観的な理由を添えて提案します。
除圧術(神経の圧迫をとるだけ)と固定術(骨をくっつける)の選択において、患者の年齢やライフスタイルに応じたデータを提示します。
- それぞれのトレードオフ: 「除圧術は手術時間が短く出血も少ないため体への負担が軽いですが、将来的にグラつきが進行して再手術になる可能性が一部あります。一方、固定術は手術の負担や合併症リスクが高まりますが、特に65歳以上の方では、より良い回復と満足度(最適な成績)を得られる確率が70%高まるという研究結果があります」と具体的な数値を示します。
- 共有意思決定(SDM): 「治療の成功とは、単に画像が綺麗になることではなく、あなたが『長距離を歩けるようになりたい』のか『とにかく痛みを減らしたい』のかという目的に到達することです。
最新の研究データ(機械学習による分類など)と、あなたの価値観を照らし合わせて、一番成功率の高い方法を一緒に選びましょう」と締めくくります。
変性腰椎すべり症(DLS)の重症度予測や治療成績の向上に向けて、現状のエビデンスギャップを埋めるための今後の主要な研究課題は以下の通りです。
現在、腰椎疾患全般の遺伝性は示されているものの、変性腰椎すべり症(DLS)の発症や進行に特化した遺伝子多型やバイオマーカーは確立されていません。
- 大規模・多民族での検証: 構造タンパク質や炎症・異化に関連する遺伝子多型と変性腰椎すべり症(DLS)重症度との関連を、複数の民族集団で大規模に検証する必要があります。
- 機能的検証: 同定された多型の多くはイントロン領域にあるため、分子レベルでの遺伝子発現や機能を確認する研究が不可欠です。
- 炎症性バイオマーカー: 血液中の循環炎症性タンパク質と、動的不安定性や術後成績との関連を前向きに評価し、臨床で使える予測モデルを構築することが求められています。
- 座位撮影や屈曲伸展撮影、MRI所見(ファセット関節液や椎間板高指数など)を統合した標準化アルゴリズムを開発し、多施設で検証する必要があります。
- 動的不安定性と術後成績の関連を前向きに評価し、どの程度であればどの術式が良いかという臨床的有用性を明確にすることが課題です。
現在ある術後成績(除圧単独と固定術追加の比較など)のデータの多くは、追跡期間が2年以内のものに偏っています。
- 超長期の追跡: 10年以上の長期的な再手術率、隣接椎間板障害の発生率、および患者の生活の質(PRO)の経時的変化を、多施設共同の前向きレジストリで蓄積する必要があります。
- 特に無症候性の偽関節などは定期的な画像検査がないと見逃されるため、標準化されたプロトコルでの長期追跡が求められます。
うつ症状や運動恐怖が治療成績の強力な予測因子であることは判明していますが、それらに対する介入が実際に成績を向上させるかのエビデンスが不足しています。
- 認知行動療法、運動療法、患者教育などの介入が、術後成績を改善できるかを検証するランダム化比較試験が必要です。
- 介入の最適なタイミング(術前か術後か)や、強度、費用対効果の評価も求められています。
現在の予測モデルは特定の変数に依存しており、予測精度にはまだ改善の余地があります。
- 生体力学的パラメータ、画像所見、心理社会的因子、そして遺伝的因子をすべて統合した包括的な予測モデルの開発が必要です。
- 開発されたモデルは、他の独立した患者群でも機能するか(外部検証)を確認し、実際の臨床現場で「意思決定支援ツール」として使った場合に有効かをランダム化比較試験で実証する必要があります。
これらの課題を解決するためには、大規模なデータの統合が不可欠です。
- 国際レジストリの構築: 多様な民族集団における予測因子の普遍性と特異性を評価するため、国際共同レジストリの構築とデータ共有プラットフォームが必要です。
- 評価の標準化: ODIやVASなどの患者報告アウトカムは広く使われていますが、評価するタイミングや「意味のある改善(MCID)」の定義が研究間で異なるため、国際的なコンセンサスに基づいた標準化が求められています。
これらの体系的な研究が進むことで、単に画像を治すだけでなく、患者一人ひとりの特性(臨床表現型)に合わせた最適な治療法を提供する**個別化医療(精密医療)**の実現が期待されています。
変性腰椎すべり症(DLS)の重症度予測因子に関する包括的レビューの結論は、**「多面的評価の重要性」と「個別化医療(精密医療)への展望」**に集約されています。
具体的な結論のポイントは以下の通りです。
高いL3屈曲角や矢状面垂直軸(SVA)、動的不安定性といった指標は、「保存療法が失敗しやすい」ことを予測する有用なサインであり、これらを持つ患者には早期の手術検討が推奨されます。
さらに、これらの予測因子のエビデンスを用いて、画像と実際の症状との関連を分かりやすく説明し、治療の利点と欠点(例えば、重症患者は術後の「改善幅」は大きいが、「絶対的なスコア」は劣る傾向があることなど)を提示することで、患者の現実的な期待値管理と、共有意思決定(Shared Decision Making)が促進されると結論づけています。
現状の課題として、変性腰椎すべり症(DLS)特異的な遺伝的バイオマーカーの不足、動的不安定性の定義の標準化の欠如、10年以上の長期予後データの不足、心理社会的介入に関するエビデンス不足などが指摘されており、これらを埋める国際共同研究やデータ共有が求められています。
その上で、臨床現場では脊椎外科医、放射線科医、理学療法士、心理士などの多職種が連携し、身体的だけでなく術前の心理的スクリーニングを含めた包括的な評価と介入を行うことが、最良の成績をもたらすと強調されています。こうしたエビデンスに基づくアプローチを実践することで、変性腰椎すべり症(DLS)患者の生活の質(QOL)向上と医療資源の効率的な活用が実現できると結ばれています。
[1]Z. Liu, G. Dai, Y. Cao, and C. Duan, “Analysis of Degenerative and Isthmic Lumbar Spondylolisthesis from the Difference of Pelvic Parameters and the Degree of Degeneration through Imaging Data,” Journal of Personalized Medicine, Sept. 2023, doi: 10.3390/jpm13091420.
[2]W. Slikker et al., “Image-Based Markers Predict Dynamic Instability in Lumbar Degenerative Spondylolisthesis,” vol. 17, no. 1, pp. 221–227, Mar. 2020, doi: 10.14245/NS.1938440.220.
[3]M. C. Snoddy et al., “Can facet joint fluid on MRI and dynamic instability be a predictor of improvement in back pain following lumbar fusion for degenerative spondylolisthesis,” European Spine Journal, vol. 25, no. 8, pp. 2408–2415, Apr. 2016, doi: 10.1007/S00586-016-4525-1.
[4]I. Radovanovic et al., “Influence of postoperative sagittal balance and spinopelvic parameters on the outcome of patients surgically treated for degenerative lumbar spondylolisthesis.,” Journal of Neurosurgery, vol. 26, no. 4, pp. 448–453, Jan. 2017, doi: 10.3171/2016.9.SPINE1680.
[5]“The L3 Flexion Angle Predicts Failure of Non-Operative Management in Patients with Tandem Spondylolithesis,” Global Spine Journal, pp. 219256822311613–219256822311613, Mar. 2023, doi: 10.1177/21925682231161305.
[6]P. Köhli et al., “The Relationship Between Paraspinal Muscle Atrophy and Degenerative Lumbar Spondylolisthesis at the L4/5 Level.,” The Spine Journal, Apr. 2024, doi: 10.1016/j.spinee.2024.03.016.
[7]R. Wang et al., “Risk factors analysis and predictive model of degree I degenerative lumbar spondylolisthesis,” Journal of Orthopaedic Surgery and Research, vol. 19, no. 1, Dec. 2024, doi: 10.1186/s13018-024-05346-y.
[8]G. Camino-Willhuber et al., “Severe Intervertebral Vacuum Phenomenon is Associated With Higher Preoperative Low Back Pain, ODI, and Indication for Fusion in Patients With Degenerative Lumbar Spondylolisthesis,” Clinical spine surgery, vol. 37, no. 1, pp. E1–E8, Aug. 2023, doi: 10.1097/bsd.0000000000001510.
[9]D.-F. Wang, X. Chen, D. Han, C. Kong, and S. Lu, “The effect of sagittal alignment, coronal balance, and segmental stability on preoperative patient-reported outcomes in patients with degenerative lumbar spondylolisthesis,” BMC Surgery, vol. 23, no. 1, Mar. 2023, doi: 10.1186/s12893-023-01947-2.
[10]E. Yang et al., “What factors predict the best outcomes for older patients operated on for grade I degenerative lumbar spondylolisthesis? A machine learning analysis from the Quality Outcomes Database.,” pp. 1–12, Jan. 2026, doi: 10.3171/2025.8.spine25945.
[11]鄔恒斐 et al., “腰椎滑脫病人術前失能情形及其影響因素探討 Preoperative Disability and Its Influencing Factors in Patients With Lumbar Spondylolisthesis,” Jan. 2018.
[12]“Preoperative Factors Affecting the Two-Year Postoperative Outcome in Single-Level Lumbar Grade I Degenerative Spondylolisthesis: Prospective, Multicenter, Patient-Preference Cohort Study using Patient-Reported Assessment,” Sept. 2022, doi: 10.21203/rs.3.rs-2015621/v1.
[13]L. Zhang, “Does the change of pelvic incidence predict the listhesis progression among pediatric patients with Low-Grade Spondylolisthesis,” Jan. 2023, doi: 10.21203/rs.3.rs-2458268/v1.
[14]S. K. M. L, D. Sharma, and J. Menon, “Prognostic Importance of Spinopelvic Parameters in the Assessment of Conservative Treatment in Patients with Spondylolisthesis.,” Asian Spine Journal, vol. 12, no. 2, pp. 277–284, Apr. 2018, doi: 10.4184/ASJ.2018.12.2.277.
[15]I. Ogon, “Factors associated with low back pain in patients with lumbar spinal stenosis: a cross-sectional study,” BMC Musculoskeletal Disorders, vol. 23, no. 1, June 2022, doi: 10.1186/s12891-022-05483-7.
[16]O. Gille et al., “A new classification system for degenerative spondylolisthesis of the lumbar spine.,” European Spine Journal, vol. 26, no. 12, pp. 3096–3105, Aug. 2017, doi: 10.1007/S00586-017-5275-4.
[17]W. Pan et al., “Lumbar alignment and patient-reported outcomes after single-level transforaminal lumbar interbody fusion for degenerative lumbar spondylolisthesis with and without local coronal imbalance,” Journal of Neurosurgery, vol. 1, no. 3, pp. 1–7, Mar. 2021, doi: 10.3171/2020.7.SPINE20703.
[18]W. Da et al., “Quantitative Analysis of Relationship Between Paraspinal Muscle Degeneration and Degree of Degenerative Lumbar Spondylolisthesis.”, doi: 10.1097/brs.0000000000005270.
[19]T. Yoshihara et al., “Analyzing lumbar vertebral shape and alignment in female patients with degenerative spondylolisthesis: Comparisons with spinal stenosis and risk factor exploration,” PLOS ONE, vol. 19, Apr. 2024, doi: 10.1371/journal.pone.0301974.
[20]“Radiographic analysis of dynamic lumbar motion during the five-repetition sit-to-stand test in degenerative lumbar spondylolisthesis,” Apr. 2022, doi: 10.21203/rs.3.rs-1574888/v1.
[21]M.-S. Moon, M.-K. Yoon, K.-T. Kwon, M.-S. Park, B.-K. Park, and S.-S. Kim, “Posterior element morphology and degenerative lumbar spondylolisthesis,” Journal of Musculoskeletal Research, vol. 18, no. 01, p. 1550001, July 2015, doi: 10.1142/S0218957715500013.
[22]P. Rahardjo, H. W. Utama, R. Setiawati, and D. Tinduh, “Correlation of the Risk Factors in Degenerative Lumbar Spondylolisthesis with MRI Imaging,” July 2023, doi: 10.47836/mjmhs.19.4.23.
[23]R. Liu, T. He, X. Wu, W. Tan, Z. Yan, and Y. Deng, “Biomechanical response of decompression alone in lower grade lumbar degenerative spondylolisthesis--A finite element analysis,” Journal of Orthopaedic Surgery and Research, vol. 19, Apr. 2024, doi: 10.1186/s13018-024-04681-4.
[24]“Correlation between the spinopelvic type and morphological characteristics of lumbar facet joints in degenerative lumbar spondylolisthesis,” Journal of neurosurgery, vol. 38, no. 4, pp. 425–435, Apr. 2023, doi: 10.3171/2022.11.spine22979.
[25]Z. Wang et al., “Radiographic risk factors for degenerative lumbar spondylolisthesis: A comparison with healthy control subjects,” Frontiers in Surgery, vol. 9, Oct. 2022, doi: 10.3389/fsurg.2022.956696.
[26]N. D. Hung, N. M. Duc, N.-T. Hang, N. T. P. Anh, N. D. Minh, and N. D. Hue, “The efficacy of quantitative magnetic resonance imaging in the diagnosis of unstable L4/L5 degenerative spondylolisthesis,” Biomedical Reports, vol. 17, no. 2, June 2022, doi: 10.3892/br.2022.1550.
[27]S. F. Elmose, M. O. Andersen, F. G. Sigmundsson, and L. Y. Carreon, “Magnetic Resonance Imaging Proxies for Segmental Instability in Degenerative Lumbar Spondylolisthesis Patients,” Spine, vol. 47, pp. 1473–1482, July 2022, doi: 10.1097/BRS.0000000000004437.
[28]N. D. Nguyen, H. Vu, T. T. H. Nguyễn, and H. M. Le, “Triệu chứng lâm sàng, hình ảnh trượt đốt sống thắt lưng do thoái hóa ở bệnh nhân bị đái tháo đường type ii,” Tạp chí Y học Việt Nam, vol. 539, no. 1, June 2024, doi: 10.51298/vmj.v539i1.9730.
[29]Z. Zhang, M. Tantai, H. Ma, S.-F. Yu, B. Chen, and Z. Lü, “Analysis of Risk Factors for Lumbar Spondylolisthesis: A Logistic Regression Study,” World Neurosurgery, pp. 123931–123931, Mar. 2025, doi: 10.1016/j.wneu.2025.123931.
[30]C. De and C. De, “Impact of Concomitant Spinal Canal Stenosis on Clinical Presentation of Adult Onset Degenerative Lumbar Spondylolisthesis: A Study Combining Clinical and Imaging Spectrum,” Cureus, vol. 13, no. 11, Nov. 2021, doi: 10.7759/CUREUS.19536.
[31]R. S. Perera, “Role of lumbar disc degeneration and genetic variation in chronic low back pain,” Ceylon Journal of Medical Science, vol. 55, no. 1, p. 3, Aug. 2018, doi: 10.4038/CJMS.V55I1.4931.
[32]A. Omair et al., “Age and pro-inflammatory gene polymorphisms influence adjacent segment disc degeneration more than fusion does in patients treated for chronic low back pain.,” European Spine Journal, vol. 25, no. 1, pp. 2–13, Jan. 2016, doi: 10.1007/S00586-015-4181-X.
[33]Q. Zheng, R. Lin, D. Wang, Z. Cui, and X. Wang, “Effects of circulating inflammatory proteins on spinal degenerative diseases: Evidence from genetic correlations and Mendelian randomization study,” JOR spine, vol. 7, no. 2, June 2024, doi: 10.1002/jsp2.1346.
[34]O. S. Akbik, V. S. Ban, M. C. MacAllister, S. G. Aoun, and C. A. Bagley, “Genetic and serum markers in adult degenerative scoliosis: a literature review.,” Spine deformity, Nov. 2021, doi: 10.1007/S43390-021-00451-Y.
[35]P. Shahi et al., “Clinical and Radiological Predictors of Slower and Non-Improvement Following Surgical Treatment of L4-5 Degenerative Spondylolisthesis: Preliminary Results.,” Spine, Apr. 2024, doi: 10.1097/brs.0000000000005019.
[36]S. Dong et al., “Evaluation of the Predictors for Unfavorable Clinical Outcomes of Degenerative Lumbar Spondylolisthesis After Lumbar Interbody Fusion Using Machine Learning,” Frontiers in Public Health, vol. 10, Mar. 2022, doi: 10.3389/fpubh.2022.835938.
[37]F. Y. Hijji et al., “Risk Factors Associated With Failure to Reach Minimal Clinically Important Difference in Patient-reported Outcomes Following Minimally Invasive Transforaminal Lumbar Interbody Fusion for Spondylolisthesis.,” Clinical spine surgery, vol. 31, no. 1, Feb. 2018, doi: 10.1097/BSD.0000000000000543.
[38]M. J. McGirt et al., “An analysis from the Quality Outcomes Database, Part 1. Disability, quality of life, and pain outcomes following lumbar spine surgery: predicting likely individual patient outcomes for shared decision-making.,” Journal of Neurosurgery, vol. 27, no. 4, pp. 357–369, Oct. 2017, doi: 10.3171/2016.11.SPINE16526.
[39]I. Khosla et al., “Severe Preoperative Disability Is Associated with Greater Mental Health Improvements Following Surgery for Degenerative Spondylolisthesis: A Cohort Matched Analysis.,” Neurospine, Jan. 2024, doi: 10.14245/ns.2347080.540.
[40]J. Zhang et al., “Role of Paraspinal Muscle Degeneration as a Predictor of Chronic Low Back Pain in Lumbar Spondylolisthesis: A Machine Learning Model is Developed,” Global Spine Journal, Sept. 2025, doi: 10.1177/21925682251383166.
[41]V. Moorthy, G. S. Goh, and R. C. C. Soh, “What Preoperative Factors Are Associated With Achieving a Clinically Meaningful Improvement and Satisfaction After Single-Level Transforaminal Lumbar Interbody Fusion for Degenerative Spondylolisthesis?,” Global Spine Journal, pp. 21925682221139816–21925682221139816, Nov. 2022, doi: 10.1177/21925682221139816.
[42]A. K. Chan et al., “Predictors of the Best Outcomes Following Minimally Invasive Surgery for Grade 1 Degenerative Lumbar Spondylolisthesis.,” Neurosurgery, vol. 87, no. 6, pp. 1130–1138, Nov. 2020, doi: 10.1093/NEUROS/NYAA206.
[43]F. N. Anwar et al., “Worse Pain and Disability at Presentation Predicts Greater Improvement in Pain, Disability, and Mental Health in Patients Undergoing Minimally Invasive Transforaminal Lumbar Interbody Fusion for Degenerative Spondylolisthesis,” Clinical spine surgery, June 2024, doi: 10.1097/bsd.0000000000001650.
[44]A. Abbas, K. Pedro, C. Bailey, J. Uruqhurt, G. McIntosh, and R.-A. Glennie, “Machine learning-driven clinical and imaging clustering of degenerative lumbar spondylolisthesis: implications for stratified surgical care,” Orthopaedic proceedings/Journal of bone and joint surgery. British volume. Orthopaedic proceedings, vol. 108-B, no. SUPP_1, pp. 113–113, Jan. 2026, doi: 10.1302/1358-992x.2026.1.113.
[45]B. Tunç, O. Uzlu, Ö. F. Şahin, E. ÜNAL, A. Yılmaz, and E. Çağıl, “Sleep and Quality of Life Before and After Surgery in Patients with Low-Grade Lumbar Spondylolisthesis,” Medical Science Monitor, vol. 31, Nov. 2025, doi: 10.12659/msm.950921.
[46]C. Guo, F. Liu, H. Liu, F. Sun, and S. Xu, “Decompression, decompression plus fusion and decompression plus dynamic stabilization for degenerative lumbar spondylolisthesis: a network meta-analysis.,” Journal of Orthopaedic Surgery and Research, Dec. 2025, doi: 10.1186/s13018-025-06550-0.
[47]A. C. Glendenning, R. Richards, S. Singh, and A. Khurana, “Surgical management of lumbar stenosis in the presence of degenerative spondylolisthesis: are decompression and fusion or interspinous process device superior to decompression alone? a systematic review and meta-analysis,” Orthopaedic Proceedings, vol. 105-B, no. SUPP_4, pp. 18–18, Mar. 2023, doi: 10.1302/1358-992x.2023.4.018.
[48]R. Kaiser et al., “Decompression alone versus decompression with instrumented fusion in the treatment of lumbar degenerative spondylolisthesis: a systematic review and meta-analysis of randomised trials,” Journal of Neurology, Neurosurgery, and Psychiatry, p. jnnp-330158, Feb. 2023, doi: 10.1136/jnnp-2022-330158.
[49]L. Schönnagel et al., “Decision-making Algorithm for the Surgical Treatment of Degenerative Lumbar Spondylolisthesis of L4/L5.,” Spine, June 2023, doi: 10.1097/BRS.0000000000004748.
[50]A. K. Chan et al., “Laminectomy alone versus fusion for grade 1 lumbar spondylolisthesis in 426 patients from the prospective Quality Outcomes Database.,” Journal of Neurosurgery, vol. 30, no. 2, pp. 234–241, Feb. 2019, doi: 10.3171/2018.8.SPINE17913.
[51]E. F. Bisson et al., “Patient-reported outcome improvements at 24-month follow-up after fusion added to decompression for grade I degenerative lumbar spondylolisthesis: a multicenter study using the Quality Outcomes Database.,” Journal of Neurosurgery, vol. 35, no. 1, pp. 1–10, Apr. 2021, doi: 10.3171/2020.9.SPINE201082.
[52]M. C. Gerling et al., “Risk Factors for Reoperation in Patients Treated Surgically for Degenerative Spondylolisthesis: A Subanalysis of the 8-year Data From the SPORT Trial.,” Spine, vol. 42, no. 20, pp. 1559–1569, Oct. 2017, doi: 10.1097/BRS.0000000000002196.
[53]H. Jia, Z. Zhang, J. Qin, L. Bao, J. Ao, and H. Qian, “Management for degenerative lumbar spondylolisthesis: a network meta-analysis and systematic review basing on randomized controlled trials.,” International Journal of Surgery, Mar. 2024, doi: 10.1097/js9.0000000000001228.
[54]A. M. Pearson et al., “Spine patient outcomes research trial: radiographic predictors of clinical outcomes after operative or nonoperative treatment of degenerative spondylolisthesis.,” Spine, vol. 33, no. 25, pp. 2759–2766, Dec. 2008, doi: 10.1097/BRS.0B013E31818E2D8B.
[55]H. Inose et al., “Predictive Factors Affecting Surgical Outcomes in Patients with Degenerative Lumbar Spondylolisthesis.,” Spine, vol. 46, no. 9, pp. 610–616, May 2021, doi: 10.1097/BRS.0000000000003944.
[56]I. W. G. B. Arimbawa et al., “Comparison between Decompression Alone and with Additional Fusion for Degenerative Lumbar Spondylolisthesis: A Systematic Review and Meta-Analysis,” Spine surgery and related research, vol. 7, no. 1, pp. 42–51, Aug. 2022, doi: 10.22603/ssrr.2022-0011.
[57]M. Hjälm, “Laminectomy With Fusion is Associated With Greater Functional Improvement Compared With Laminectomy Alone for the Treatment of Degenerative Lumbar Spondylolisthesis,” Spine, vol. 48, no. 12, pp. 874–884, Apr. 2023, doi: 10.1097/brs.0000000000004673.
[58]J. F. Karp et al., “Clinical and neuropsychiatric correlates of lumbar spinal surgery in older adults: results of a pilot study.,” Pain management, vol. 6, no. 6, pp. 543–552, Apr. 2016, doi: 10.2217/PMT.16.9.
[59]J. Lee, H.-S. Kim, K.-D. Shim, and Y.-S. Park, “The Effect of Anxiety, Depression, and Optimism on Postoperative Satisfaction and Clinical Outcomes in Lumbar Spinal Stenosis and Degenerative Spondylolisthesis Patients: Cohort Study,” Clinics in Orthopedic Surgery, vol. 9, no. 2, pp. 177–183, June 2017, doi: 10.4055/CIOS.2017.9.2.177.
[60]G. Barone et al., “Spondylolisthesis in young patients: postoperative functional outcomes at 22-year mean follow-up,” Archives of Orthopaedic and Trauma Surgery, pp. 1–10, June 2021, doi: 10.1007/S00402-021-04006-8.
[61]L. Schönnagel et al., “Predicting Postoperative Outcomes in Lumbar Spinal Fusion: development of a machine learning model,” The Spine Journal, Oct. 2023, doi: 10.1016/j.spinee.2023.09.029.
[62]P. V. Mummaneni et al., “Predictive model for long-term patient satisfaction after surgery for grade I degenerative lumbar spondylolisthesis: insights from the Quality Outcomes Database.,” Neurosurgical Focus, vol. 46, no. 5, May 2019, doi: 10.3171/2019.2.FOCUS18734.
[63]M. A. MacLean et al., “Evaluating Instability in Degenerative Lumbar Spondylolisthesis,” vol. 7, Nov. 2022, doi: 10.2106/JBJS.OA.22.00052.
[64]N. Dietz et al., “Variability in the utility of predictive models in predicting patient-reported outcomes following spine surgery for degenerative conditions: a systematic review.,” Neurosurgical Focus, vol. 45, no. 5, Nov. 2018, doi: 10.3171/2018.8.FOCUS18331.
[65]“Prediction of postoperative disability in patients with degenerative diseases of the lumbar spine using preoperative psychological factors,” Mar. 2023, doi: 10.21203/rs.3.rs-2594911/v1.
[66]A. K. Chan et al., “113 Clinical Presentation Phenotypes of Patients Operated for Lumbar Spondylolisthesis: An Analysis of the Quality Outcomes Database,” Neurosurgery, vol. 68, no. Supplement_1, pp. 31–32, Mar. 2022, doi: 10.1227/neu.0000000000001880_113.
[67]D. Nasef, D. Nasef, V. Sawiris, P. Girgis, and M. Toma, “Machine-Learning-Based Biomechanical Feature Analysis for Orthopedic Patient Classification with Disc Hernia and Spondylolisthesis,” BioMedInformatics, vol. 5, no. 1, pp. 3–3, Jan. 2025, doi: 10.3390/biomedinformatics5010003.
[68]V. Quack et al., “Psychological factors outmatched morphological markers in predicting limitations in activities of daily living and participation in patients with lumbar stenosis,” BMC Musculoskeletal Disorders, vol. 20, no. 1, pp. 557–557, Nov. 2019, doi: 10.1186/S12891-019-2918-0.
[69]K. Rangwalla et al., “Degenerative lumbar spondylolisthesis: review of current classifications and proposal of a novel classification system.,” European Spine Journal, Aug. 2023, doi: 10.1007/s00586-023-07818-x.
[70]A. G. Kulkarni, T. S. Kunder, and S. Dutta, “Degenerative Spondylolisthesis: When to Fuse and When Not to? A New Scoring System.,” Clinical spine surgery, vol. 33, no. 8, Mar. 2020, doi: 10.1097/BSD.0000000000000970.
ごあいさつ

長引いた痛みを一人で治すのは困難なことが多いです。
困ったときは自身で判断せずに適切な処置を受けるために専門家に相談しましょう。
もし、お近くにお住まいで、困っているならば、一度ひまわり接骨院までお問い合わせください。腰痛・坐骨神経痛の専門家の新幡が、ご相談に乗ります。
気軽にご相談ください。

新着情報・お知らせ
お気軽にお問合せください

お電話でのお問合せ・相談予約
<受付時間>
月~土
9:00〜13:00 /15:00〜19:00
※日曜・祝日は除く
フォームは24時間受付中です。お気軽にご連絡ください。
ひまわり接骨院

住所
〒213-0002
神奈川県川崎市高津区二子1丁目7−17 リバーサイドマンション杉崎 102
アクセス
二子新地駅 徒歩3分
駐車場:近隣にコインパーキングあり。自転車・バイクは店舗前に駐輪場がございます。
受付時間
月~土
9:00〜13:00 /15:00〜19:00
定休日
日曜・祝日

