
〒213-0002 神奈川県川崎市高津区二子1丁目7−17
リバーサイドマンション杉崎 102 二子新地駅 徒歩3分
| 月 | 火 | 水 | 木 | 金 | 土 | 日祝 | |
|---|---|---|---|---|---|---|---|
| 9:00〜13:00 | ● | ● | ● | ● | ● | ● | ─ |
| 15:00〜19:00 | ● | ● | ● | ● | ● | ● | ─ |
変形性股関節症の進行と重症化を予測する因子は?
公開日:2026/07/07
更新日:2026/00/00
股関節部変形性関節症(OA)の進行と重症化を予測する因子について、多角的な視点から包括的に解説しています。
主に放射線学的画像、生物学的マーカー、運動力学的機能、臨床的背景という4つの領域における最新の研究成果が統合されています。
関節裂隙の狭小化や特定の形態異常といった画像診断指標に加え、軟骨代謝に関連する尿中・血清マーカーの有効性が示唆されています。
また、歩行速度や関節への機械的負荷といった身体機能面、および年齢や肥満度などの患者背景が、将来の機能低下や人工関節置換術への移行にどう影響するかが分析されています。
最終的に、機械学習や国際的なデータ共有を活用した個別化予測モデルの構築が、早期介入と最適な治療選択に不可欠であると結論付けています。
目次
変形性股関節症(OA)の進行と重症化を予測する因子に関する主要な知見は、**「画像診断学的」「生化学的(分子)」「バイオメカニクス(機能的)」「臨床・人口統計学的」**の4つの主要ドメインに分類され、以下のようなエビデンスが示されています。
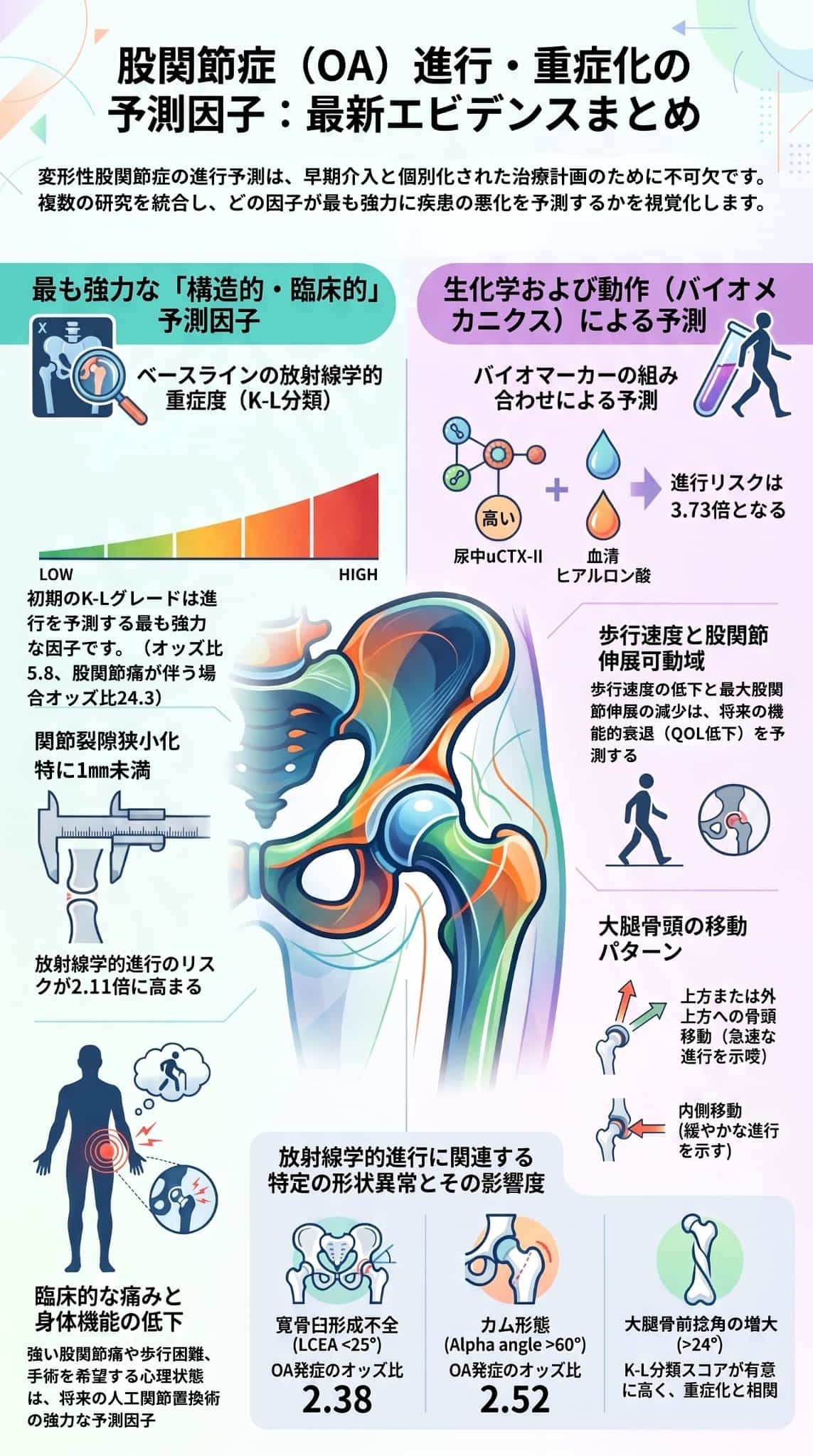
■初期のKellgren-Lawrence(K-L)グレード: ベースラインにおけるK-Lグレードは進行を予測する最も強力な因子です。1,904名を対象とした平均6.6年の追跡調査では、ベースラインでの高グレードが進行のオッズ比(OR)5.8を示し、股関節痛が伴う場合はOR 24.3まで急上昇しました。
■関節裂隙幅 (Joint Space Width: JSW) の狭小化: ベースラインで JSWが 2.5 mm 未満、あるいは特に 1.0 mm 未満であることは、将来の構造的進行の強力な予測因子です。さらに、JSW < 1.0 mm と大腿骨頭の「外上方への移動(superolateral migration)」が組み合わさると、進行のORは 4.25 に達します。
■骨盤・股関節の形態学的異常:
- **寛骨臼形成不全(LCEA < 25°)**は、股関節OAの発生リスクを著しく高めます(OR 2.38)。
- **カム変形(α角 > 60°)**もOA発生リスク(OR 2.52)と関連しますが、より高グレードへの進行予測における一貫性は形成不全に比べるとやや劣ります。
- **大腿骨の前捻角異常(> 14°、特に > 24°)**は、正常な角度の患者と比較して、有意に高いK-Lスコア(重症度)と相関しています。
■先進的な3D画像技術: 従来の2D X線画像による最小JSW測定(AUC 0.73)に対し、**「3D関節裂隙マッピング」と「統計的形状モデリング(SSM)」をK-Lグレードに組み合わせることで、将来の関節置換術の予測精度がAUC 0.86(18%の精度向上)**に達することが示されています。
- 尿中CTX-II(uCTX-II): 最も広く研究されている軟骨分解マーカーであり、高値は関節裂隙の減少や人工股関節置換術への進行を予測します。特に急速に進行する**急速破壊型股関節症(RDA)**において予測価値が高く、尿中Helix-IIと双方が高いレベルにある場合、RDAのオッズ比は非常に高くなります(uCTX-II: OR 6.67、Helix-II: OR 5.73)。
- 血清ヒアルロン酸(HA): 滑膜炎症マーカーである血清HAも構造的進行と関連しており、uCTX-IIと血清HAの双方が最も高いグループに属する場合、進行の相対リスクは 3.73 に上昇します。
- 関連が薄いと判断されているマーカー: 血清COMPについては予測価値に関する矛盾した結果が報告されており、骨代謝マーカー(CTX-I、NTX-I、PINP、PIIINPなど)にいたっては、画像上の進行と関連がないという強いエビデンスが存在します。
- 歩行速度 (Gait Speed): ベースラインの歩行速度の低下は、HOOS(股関節障害・変形性関節症成果スコア)における症状や強直、痛みの悪化といった機能低下の強力な予測因子です。逆に、歩行速度が速い患者は、将来の人工股関節置換術へと進行する確率が低くなります(ハザード比 0.64)。
- 最大股関節伸展角度: 歩行時の最大股関節伸展角度の減少は、HOOSの「スポーツ・余暇活動」や「QOL」スコアの低下といった、将来の主観的機能低下を予測します。
- 累積的な関節負荷 (Cumulative Hip Joint Loading): 1歩ごとの股関節負荷に1日の平均歩数を掛け合わせた「日々の累積股関節負荷」が高い患者は、将来的に画像上の進行をたどりやすいことが prospective 研究で示されています。
- 脊椎アライメントと可動性: 立位での脊椎の前傾(Anterior spinal inclination)や、胸腰椎の可動性低下が、股関節にかかる負荷分布を変化させ、進行リスクに悪影響を及ぼすことが示唆されています。
日常の診療現場で最も簡便に取得できる患者情報です。
- ベースラインの臨床的重症度: 初期の股関節痛の強さ、Lequesne指数スコア≧10、および患者自身の「手術への強い希望」は、人工股関節全置換術への移行を予測するきわめて強力な臨床指標です。
- 年齢と性別: 高齢(65歳以上、あるいは発症年齢の高齢化)や、男性であること は、より早い手術への進行や急速な画像上の進行と関連しています。
- BMI(肥満度): 意外にも、BMIと「初回の関節置換術」や「画像上の進行」との直接的な関連性を否定する強いエビデンスが複数存在します。しかし、**片側の人工股関節置換術を終えた患者においては、対側の股関節OA進行(対側置換術の必要性:OR 1.1)**を予測する主要な因子であり、症状の不良な経過軌跡にも大きく関与しています。
- 合併症のパラドックス: 合併症が多いほど「臨床的(自覚症状など)な進行」は加速する一方で、「人工股関節手術(THR)への移行」は逆に遅くなるというデータがあります(3つ以上の合併症保有者でHR 0.62)。これは疾患そのものの性質ではなく、手術適応から除外されやすいという医療現場の選択バイアスを反映している可能性が指摘されています。
- 人種による進行パターンの違い: 例えばアフリカ系アメリカ人は可動域制限や障害などの機能的な進行を示しやすく、白人は画像上の(骨の)進行を示しやすいなど、人種集団によってOAの進行経路に異なるパターンが存在することが示されています。
臨床において最も信頼性が高く再現性のある進行予測因子は、**「ベースライン時の画像上の重症度(K-Lグレード、JSW狭小化)」「大腿骨頭の移動パターン(外上方)」「ベースライン時の疼痛や臨床症状の重さ」**です。
現在、予測精度を高めるためにこれら複数のドメイン(画像、臨床、バイオ、遺伝学)の個別データを統合し、人工知能(AI)を活用して個別化された進行予測ツールを開発する世界的な共同プロジェクト(World COACH consortium など)が進行しています。
変形性股関節症(OA)の進行と重症化における画像診断上の予測因子について、レントゲンや先進画像技術(MRI・3D技術)を用いた主要な知見を詳しく解説します。
従来のX線単純画像における指標は、構造的進行や人工関節置換術(THR/THA)への移行を予測する上で最も確立された因子です。
■ベースラインのKellgren-Lawrence(K-L)グレード
- ベースライン時のK-Lグレードは進行を予測する最も強力な指標の一つです。1,904名を平均6.6年間追跡した住民コホート研究では、ベースラインの高グレード群における進行のオッズ比(OR)は 5.8 であり、股関節痛を伴う場合はOR 24.3 まで跳ね上がりました。系統的レビューでも、高K-LグレードとTHRへの進行との強い関連が確認されています。
- 一方で、大腿骨頭のピストルグリップ変形や股関節インピンジメント(FAI)を有する例において、ベースラインの Tönnisグレード(1 vs 2)は10年間の進行リスクを差別化しなかった と報告されています。
■関節裂隙幅(JSW)の基準と狭小化速度
- 461名を対象とした1年間の前向き研究において、画像上の進行(JSWの0.5mm以上の減少)は全体の22%にみられ、ベースラインのJSWが 2.5 mm 未満であることが進行を予測しました。
- ベースラインJSW < 1.0 mm は、進行の独立した強力な予測因子(OR 2.11)「JSW < 1.0 mm」に「大腿骨頭の外上方への移動(superolateral migration)」が組み合わさると、進行のORは 4.25 に上昇します。
- 将来的に人工股関節置換術に至る患者の年間平均JSW狭小化速度は 0.43 ± 0.43 mm/年(中央値 0.29)であり、特に萎縮性(atrophic)OAでより急速な狭小化(r = 0.71)が認められます。
■骨頭の移動パターンおよび骨自体の変化
- 上方または外上方(superolateral)への大腿骨頭の移動、および萎縮性の骨反応は急速な進行と関連しています。これに対し、内側(medial)、軸性(axial)、または不定な移動パターンは、より緩徐な進行を示します。
- 個別の骨特徴として、軟骨下骨硬化(subchondral sclerosis)大腿骨頭骨棘、外上方関節裂隙狭小化、内側骨棘なども、画像上の進行や将来のTHR移行を予測する独立した因子であることが示されています。
■寛骨臼形成不全(Acetabular Dysplasia)
- 寛骨臼による大腿骨頭の被覆不全は、股関節OAの発症および進行の強力なリスク因子です。LCEA(外側中心骨頭角)の低下がOA発症と関連しており、LCEA < 25°の寛骨臼形成不全がある場合、股関節OA発症のオッズ比は 2.38 に達します。
■カム変形(Cam Morphology)
- α角 > 60°で定義されるカム変形は、股関節OA発症のリスクを高めますが(OR 2.52)、より重症のOAグレードへと進行させる予測因子としてのエビデンスは一貫性を欠いています(9つの研究を対象とした系統的レビューにおいて、カム変形と重症化進行の関連を示した論文は1つのみでした)。
- ピストルグリップ変形を有する股関節(10年以上追跡)では、内側近位大腿骨角(MPFA)の低下(81° vs 87°)や posterior wall sign(後壁徴候)の存在が、進行例を識別する画像特徴として挙げられています。
■大腿骨前捻角(Femoral Anteversion)
- 大腿骨前捻角は、OAの重症度と用量反応関係を示します。前捻角が正常範囲(>14°)を超える患者は正常範囲の患者に比べてK-Lスコアが有意に高く、さらに**前捻角が 24°を超える超前捻角の患者(K-Lスコア:3.69 ± 1.25)**は、14°超24°以下の患者(K-Lスコア:2.95 ± 1.09)よりも有意に高い重症度を示しました。大腿骨後捻(retroversion)にはこのような強い関連は認められていません。
■dGEMRIC(軟骨の遅延ガドリニウム造影MRI)
- 軟骨内のグリコサミノグリカン(GAG)含有量を生化学的に評価する手法です。dGEMRICインデックス(造影後に得られる指標)は、大腿骨近位部の骨形態測定値よりも、5年追跡時におけるレントゲン的な関節裂隙狭小化(JSW)の進行パターンとより強く相関することが示されています。
■定量的3次元CT画像(3D関節マッピング・形状モデリング)
- 健常高齢者263名のコホートにおいて、「3D関節裂隙マッピング(3D joint space mapping)」と「統計的形状モデリング(SSM)」をK-Lグレードに組み合わせることで、将来の人工関節置換術の予測精度が AUC 0.86 に到達しました。これは、FDA承認基準である従来の2Dレントゲンによる最小JSW測定(AUC 0.73)と比べて、予測精度が18%向上したことを意味します。
- また、この3D評価により、従来の2Dレントゲンでは死角となって観察できなかった関節領域における「非対称性」の進行傾向を捉えられるようになっています。
■ベースラインの大腿骨頸部幅(Femoral neck width)
- ベースライン時における大腿骨の頸部幅も、レントゲン的な進行アウトカムの予測因子となり得ることが示唆されています。
変形性股関節症(OA)の進行と重症化における**生化学的・分子マーカー(バイオマーカー)**は、関節の不可逆的な構造損傷が起こる前に、急速な進行リスクがある患者を同定する目的で研究が進められています。
■尿中II型コラーゲンC末端テロペプチド(uCTX-II)
- 股関節OAにおいて最も広範に研究されている軟骨分解マーカーです。
- 333名の患者を3年間追跡したコホート研究において、ベースラインのuCTX-IIレベルが最も高いグループ(上位3分位)は、関節裂隙幅の減少(0.5mm以上)や人工股関節置換術(THR)といった構造的進行を予測しました。また、高いuCTX-II値は、進行性の疼痛経過をたどることとも関連しています。
- 特に関節破壊が急速に進む**「急速破壊型股関節症(RDA)」の同定において強力な予測価値**を示します。RDA患者は、緩徐に進行する患者と比較して尿中Helix-IIレベルが71%高く、uCTX-IIとHelix-IIの双方が最も高いグループ(最高3分位)にある場合、RDAのオッズ比(OR)はHelix-IIで5.73、uCTX-IIで6.67に達しました。
■血清軟骨オリゴマーマトリックスプロテイン(COMP)
- 予測価値に関する結果は一貫していません(矛盾があります)。
- 膝や股関節のOA発生の予測因子として強いエビデンスを報告する系統的レビューがある一方で、関連が極めて小さいか方向性が矛盾しているとする報告もあります。さらに、股関節OAの進行に関する大規模な系統的レビューでは、画像上の進行とCOMPには関連がない(no association)という強いエビデンスが示されています。
■YKL-40
- 軟骨細胞や滑膜細胞から分泌される糖タンパク質ですが、多変量解析において構造的進行の独立した予測因子としては認められませんでした。
■血清ヒアルロン酸(HA)
- 滑膜炎症の指標となる血清HAの高値(上位3分位)は、構造的進行と関連していることが示されています。
- 後述の通り、軟骨分解マーカーであるuCTX-IIと組み合わせることで予測精度が向上します。
■マトリックスメタロプロテアーゼ(MMP、特にMMP-3)
- 初期段階でレントゲン上は関節裂隙の狭小化のみが観察される急速進行性股関節症において、血清MMP-3の高値がその後の急速な骨破壊を予測する因子となる可能性が示唆されています。
- ただし、多変量モデルにおいては、MMP-1やMMP-3が独立して構造的進行を予測する因子としては検出されなかったとする報告もあります。
■CTX-I, NTX-I, PINP, PIIINP など
- これらの骨代謝マーカーに関しては、股関節OAの画像上の(構造的)進行と「関連がない」という強いエビデンスが系統的レビューによって示されています。したがって、これらは進行予測において信頼性の低い指標とみなされています。
■uCTX-II + 血清HA(ヒアルロン酸)
- この2つのマーカーがともに最も高いグループ(最高3分位)に属する患者は、低いグループに比べて進行の相対リスクが 3.73 に上昇し、単一マーカーよりも予測価値が向上しました。
■uCTX-II + 尿中Helix-II
- 先述の通り、急速破壊型股関節症(RDA)という特定の深刻なフェノタイプを予測する上で、独立した強力な関連を示します。
- 絶対的進行速度の予測困難: 組み合わせアプローチであっても、個々の患者における「絶対的な進行速度」を正確に予測することはできません(関連の強さは中等度にとどまります)。
- 標準化の欠如: 多くのマーカーは限られた研究数でしか評価されておらず、測定手法やOAのフェノタイプ、アウトカムの定義(画像、機能、手術移行など)の不均一性により、メタアナリシスによる標準化が困難です。
変形性股関節症(OA)の進行と重症化において、生体力学的(バイオメカニクス)および機能的予測因子は、日常動作における動的な関節負荷や運動パターンがどのように疾患進行に寄与するかを理解する上で極めて重要です。静的な画像診断とは異なり、これらの因子は治療介入によって変更可能なターゲットとなり得る特徴を持っています。
■歩行速度 (Gait Speed) の低下:
- 股関節OA患者は健常者と比較して平均 0.26 m/s 遅く歩くことが示されており、この差は初期〜中等度(0.16 m/s の低下)に比べて重症期(0.27 m/s の低下)でより顕著になります。
- 3年間の前向きコホート研究において、ベースライン時の歩行速度の低下は、将来のHOOS(股関節障害・変形性関節症成果スコア)における「症状・強直(悪化のオッズ比 0.61、AUC=75%)」および「痛み(オッズ比 0.72、AUC=72%)」の進行(機能低下)を強力に予測しました。
- 逆に、大規模な患者レジストリデータにおいては、**歩行速度が速い患者ほど、将来的に人工股関節置換術(THR)へ移行するリスクが有意に低い(ハザード比 0.64)**ことが示されています。
■最大股関節伸展角度 (Maximum Hip Extension) の制限:
- 歩行解析において、ベースライン時における最大股関節伸展角度の減少は、将来の機能低下(HOOSにおけるスポーツ・余暇活動の悪化:オッズ比 0.78、QOLスコアの悪化:オッズ比 0.84)を予測する因子です。
- さらに、「歩行困難(Walking difficulty)」の自覚症状自体も、将来の人工関節移行へのきわめて強力な予測因子(ハザード比 2.20)となっています。
■日々の累積股関節負荷 (Daily Cumulative Hip Joint Loading):
- 1回の歩行サイクルにおける股関節への負荷(力の大きさ)に、1日の平均歩数を掛け合わせた「日々の累積股関節負荷」を算出したところ、この累積負荷が高い患者は、その後に画像上の構造的進行(関節裂隙の狭小化など)をたどりやすいことが前向き研究で確認されています。
- 表現型(フェノタイプ)のクラスター分析では、二次性股関節OA患者の約30%が、この「高い累積股関節負荷」を特徴とするグループに分類されました。このグループは、構造的異常(関節裂隙の狭小化)や脊椎アライメントの異常を特徴とする他のグループと同等に、12ヶ月後の進行リスクが高いことが示されています。これは、過剰な物理的負荷が、アライメント異常とは別の独立した経路で進行を促進することを示唆しています。
- 立位での脊椎の前傾 (Anterior Spinal Inclination) や、胸腰椎(thoracolumbar spine)の可動性低下が、股関節OAの進行を予測する因子として報告されています。
- 特に胸腰椎の可動性の低下は、複数の進行フェノタイプに共通して観察されており、これが股関節への局所的な負荷分布を偏らせ、機械的ストレスを悪化(あるいは保護的な代償作用を制限)させると考えられています。
股関節部変形性関節症(OA)の進行と重症化における臨床的および人口統計学的予測因子は、画像検査や特殊な生化学検査に頼ることなく、日常の診療現場で最も容易に取得できる極めて実用的な指標です。
患者が最初に診察を受けた時点での構造的・臨床的な重症度は、将来の進行を予測する上で最も強固で一貫したエビデンスを有しています。
- レントゲン上の重症度: ベースラインにおけるKellgren-Lawrence(K-L)グレードは、構造的進行を予測する最も強力な因子です。ベースラインのグレードが高いと進行のオッズ比(OR)は5.8となり、股関節痛が伴う場合はOR 24.3まで跳ね上がります。また、定量的な関節裂隙幅(JSW)が 1.0 mm未満であることも、将来の画像上の進行を強力に予測します(OR 2.11)。
- 初期の症状負担: 患者が訴える股関節痛の強さや、Lequesne指数スコアが10以上であることは、将来の進行と強く関連しています。さらに、患者自身の**「手術に対する強い希望(desire for surgery)」**は、2年以内に人工関節置換術(THR)へ移行することのきわめて強力な予測因子(ハザード比 [HR] 3.12)となります。
- 年齢: ベースライン時の年齢が 65歳超であること、または自覚症状が出現した年齢(発症年齢)が遅いことは、画像上の急速な進行を予測します。ただし、人工股関節置換術(THR)への移行に対する「年齢」の直接的な影響については研究間で結果に矛盾があり、これは合併症や個人の意思決定といった他因子の影響を強く受けるためと考えられます。
- 性別: 手術を視野に入れた運動療法コホートの分析において、男性であることは2年以内のTHRへのより急速な進行を予測する因子(HR 1.43)として示されています。
- 構造的な進行(初発)には関連が薄い: 複数の系統的レビューや大規模コホート研究(Johnston Countyコホートなど)において、**BMIは画像上の(レントゲン的な)進行や、初回の人工関節置換術への移行とは「関連がない(no association)」**という強いエビデンスが示されています。
- 対側(反対側)の進行や症状悪化には関連: 一方で、すでに片側の人工股関節置換術を終えた患者においては、**高いBMIが「対側(もう片方)の股関節」の進行および人工関節置換術の必要性を予測する有意な因子(OR 1.1)**となります。また、肥満は痛みの悪化など「好ましくない臨床症状の経過軌跡(trajectory)」を予測する主要な因子でもあります。
患者が抱える合併症は、自覚症状の進行を早める一方で、手術へのアクセスには逆の影響を及ぼします。
- 臨床的な進行の加速: 合併症の多さは、痛みや身体機能障害といった「臨床的な進行」を予測します。
- 手術移行の遅延(選択バイアス): 非常に興味深いことに、合併症が多い患者(3つ以上でHR 0.62、4つ以上でHR 0.64)ほど、人工股関節手術への移行速度が有意に遅いことが示されています。これは、変形性関節症の生物学的進行が遅いわけではなく、合併症が多い患者は全身状態の懸念から「手術適応から除外されやすい」という、医療現場における治療選択バイアスを反映していると考えられます。
- 術後の機能回復への悪影響: 術前に腰痛や対側の股関節OAなどの筋骨格系合併症を抱えている患者は、人工関節置換術の術後に得られる長期的な機能回復(WOMACなどの機能評価)が不良になりやすいことが報告されています。
「Johnston County Osteoarthritis Project」コホートは、人種によって股関節OAの進行パターンに明確な違いがあることを明らかにしました。
- アフリカ系アメリカ人: 画像上の変化よりも、**関節可動域(ROM)の消失や生活機能障害(disability)といった「機能的・臨床的な進行」**を示しやすい特徴があります。実際、関節裂隙狭小化(JSN)が生活機能障害の悪化と有意に関連するのは、アフリカ系アメリカ人のみでした。
- 白人(Caucasians): 主にレントゲン画像上で観察される**「構造的(画像上)な進行」**を示しやすい特徴があります。例えば、外側骨棘の存在が関節可動域の減少と関連するのは白人のみであることが示されています。
股関節部変形性関節症(OA)の進行と重症化の予測因子は、多岐にわたる研究によってその領域が明らかにされてきました。これら予測因子の総括と、それらがもたらす臨床的意義および今後の課題について解説します。
進行と重症化を予測することには、主に以下の3つの臨床的意義があります。
- 早期介入とリスク層別化 (Early Intervention & Risk Stratification): 進行リスクの高い患者を早期に同定することで、早期段階からターゲットを絞った適切な管理戦略(運動療法、生活指導、あるいは早期の手術検討など)を開始し、疾患の悪化を防ぐことができます。
- 臨床試験デザインの最適化 (Clinical Trial Design): 将来的に疾患修飾薬(DMOADs)が利用可能となった際、その治療効果を最も検証・獲得しやすい「急速に進行するリスクの高い集団」を正確に特定し、効率的な治験をデザインするために不可欠な情報となります。
- 非進行者(低リスク群)への安心感の提供 (Patient Reassurance): 進行のリスクが極めて低いと評価された患者に対しては、「数年間は急激に悪化しない可能性が高い」という科学的根拠に基づいた説明をすることで、患者の不要な不安を和らげ、不必要な医療利用を削減できます。
現時点におけるエビデンスを元に、臨床医は外来診療において以下のような患者指導(カウンセリング)を行うことが推奨されます。
- 高リスク患者へのカウンセリング: 初診時に、大腿骨頭の外上方(superolateral)への移動、軟骨下骨硬化(subchondral sclerosis)、そして強い股関節痛が伴っている患者は、急速に進行して将来的に人工股関節置換術(THR)に至るリスクが高いことを前提にした治療計画を立てる必要があります。
- 低リスク患者へのカウンセリング: 逆に関節裂隙の狭小化が軽度で、骨頭の移動パターンが内側(medial)であり、自覚症状が少ない(または無症状の)患者については、長期(8年程度)にわたって急速に悪化する可能性は低いと説明することができます。
実臨床にこれらの知見を組み込む上では、いくつかの大きな障壁が存在します。
- 変更不可能な因子の多さ (Non-modifiable Predictors): 現在確立されている強力な因子の多く(画像上の初期変形、年齢、性別など)は、診断時にすでに確定しており治療によって「変更不可能」なものです。そのため、予防や治療の標的(modifiable targets)となり得る「日々の累積股関節負荷」や「脊椎アライメント」といった生体力学的な要因をさらに究明することが求められています。
- 予測精度の限界 (Unexplained Variance): 複数のパラメータを組み合わせた先進的な多因子モデルであっても、その判別能(c-index)は約0.70にとどまり、進行リスクの約30%は依然として未解明のまま残されています。
- コスト、普及、標準化の壁: 3D関節裂隙マッピングやdGEMRIC(MRI造影)といった高度な先進画像技術は優れた予測精度(AUC 0.86など)を示しますが、高額な設備や専門知識を要するため日常診療には容易に導入できません。生化学マーカーも同様に、コホート間での測定の標準化やフェノタイプの検証が不足しています。
- 治療決定(手術)バイアス: 合併症(併存疾患)が多い患者ほど、人工股関節手術への移行速度が有意に遅いという「逆説的なデータ(HR 0.62)」が示されています。これは、股関節症自体の生物学的進行が遅いわけではなく、「全身状態の懸念から手術適応から外されやすい」という現場の治療選択バイアスを反映したものであり、疾患本来の経過予測を困難にしています。
現在、これらの限界を打破するために、世界的な共同プロジェクトである**「World COACHコンソーシアム」**が世界9つのコホートから38,021名分の個別データを集約し、臨床・画像・生化学・遺伝情報を調和させた個別化予測モデルの構築・検証を進めています。また、単純レントゲンと臨床情報をAIに学習させる機械学習モデルの活用も、複雑な因子の絡み合いを解明する糸口として注目されています。
股関節部変形性関節症(OA)の進行・重症化リスク予測における最終的な結論と臨床的意義は以下の通りです。
現時点で、最も科学的根拠が強固であり、複数のコホート研究で高い再現性を有しているのは**「ベースライン時の画像上の構造的重症度」と「初期の臨床症状の重さ」**です。
- 画像指標: レントゲン検査におけるKellgren-Lawrence(K-L)グレード、大腿骨頭の移動パターン(特に上方・外上方への移動)、および**軟骨下骨硬化(subchondral sclerosis)**が、最も信頼性の高い構造的進行の予測因子です。
- 臨床指標: 初診時の股関節痛の強さや、Lequesne指数スコアが10以上であることが、その後の良好でない経過や重症化と強く関連しています。
- 生化学的マーカー: 軟骨分解マーカーである尿中CTX-II(特に血清ヒアルロン酸との組み合わせ)が最も有望視されていますが、関連の強さは中等度にとどまり、個々の患者における絶対的な進行速度を予測することは困難です。
- 先進画像技術: **3D関節裂隙マッピングと統計的形状モデリング(SSM)を組み合わせることで、将来の人工関節置換術の予測精度(AUC)が従来の2D X線の0.73から0.86へと大幅に向上(18%の改善)**することが実証されています。しかし、高額な設備や専門知識を要するため、日常診療への普及には標準化や利用可能性の壁があります。
- 生体力学的(バイオメカニクス)因子: 歩行速度や最大股関節伸展角度は機能低下の軌跡を予測する上で有用ですが、多くの歩行解析研究は横断的であり、動作異常が進行の「原因」なのか「結果」なのかという因果関係の特定には至っていません。
現在の多因子予測モデルは、様々なドメインの情報を統合しても判別能(c-index)は約0.70付近にとどまっており、進行リスクの約30%は依然として未解明(説明不可能)なまま残されています。
この限界を克服するために、以下の3つの優先アプローチが世界的に進められています。
- 国際共同コンソーシアム(World COACH): 世界9つのコホートから38,021名の個別データを統合し、臨床・画像・生化学・遺伝情報を調和させた、個別化予測モデルの検証を行っています。
- 人工知能(AI)の活用: 単純X線写真と臨床データを統合し、従来の統計手法では捉えきれなかった複雑な因子間の相互作用を自動で検出・予測する機械学習モデルの開発が進められています。
- 変更可能な予測因子の追究: 日常の「累積的な股関節負荷」や「脊椎アライメント」といった、リハビリ等の介入によって変更可能な動作因子の解明に焦点が移りつつあります。
臨床医は、患者に対して科学的根拠に基づいた以下の見通し(カウンセリング)を提供することが推奨されます。
- 高リスク群: ベースラインで大腿骨頭の外上方移動、骨硬化、萎縮性の骨反応、および強い疼痛が認められる場合は、進行リスクが高く、将来的に人工股関節置換術(THR)が必要になる可能性が高いことを念頭に置き、早期から厳密な管理を行います。
- 低リスク群: 関節裂隙の狭小化が軽度で、骨頭の移動が内側(medial)であり、自覚症状が少ない(または無症状の)患者に対しては、長期的(最大8年間)にわたって急激に悪化する可能性は低いと説明し、不要な不安を和らげることができます。
[1]C. H. Teirlinck, D. M. J. Dorleijn, P. K. Bos, J. B. M. Rijkels-Otters, S. M. A. Bierma-Zeinstra, and P. A. J. Luijsterburg, “Prognostic factors for progression of osteoarthritis of the hip: a systematic review,” Arthritis Research & Therapy, vol. 21, no. 1, pp. 1–19, Aug. 2019, doi: 10.1186/S13075-019-1969-9.
[2]A. A. Wright, C. Cook, and J. H. Abbott, “Variables associated with the progression of hip osteoarthritis: A systematic review,” Arthritis & Rheumatism, vol. 61, no. 7, pp. 925–936, July 2009, doi: 10.1002/ART.24641.
[3]B. Foley, B. Foley, R. J. Cleveland, J. B. Renner, J. M. Jordan, and A. E. Nelson, “Racial differences in associations between baseline patterns of radiographic osteoarthritis and multiple definitions of progression of hip osteoarthritis: the Johnston County Osteoarthritis Project,” Arthritis Research & Therapy, vol. 17, no. 1, pp. 366–366, Dec. 2015, doi: 10.1186/S13075-015-0806-Z.
[4]M. C. C. Betancourt et al., “Dual energy x-ray absorptiometry analysis contributes to the prediction of hip osteoarthritis progression,” Arthritis Research & Therapy, vol. 11, no. 6, pp. 1–8, Nov. 2009, doi: 10.1186/AR2845.
[5]S. Clausen et al., “Prognostic factors of total hip replacement during a 2-year period in participants enrolled in supervised education and exercise therapy: a prognostic study of 3657 participants with hip osteoarthritis.,” Arthritis Research & Therapy, vol. 23, no. 1, pp. 235–235, Sept. 2021, doi: 10.1186/S13075-021-02608-6.
[6]M. Dougados et al., “Radiological progression of hip osteoarthritis: definition, risk factors and correlations with clinical status.,” Annals of the Rheumatic Diseases, vol. 55, no. 6, pp. 356–362, June 1996, doi: 10.1136/ARD.55.6.356.
[7]Z. Fan et al., “The prevalence of hip osteoarthritis: a systematic review and meta-analysis,” Arthritis Research & Therapy, vol. 25, no. 1, Mar. 2023, doi: 10.1186/s13075-023-03033-7.
[8]“Progression to arthroplasty surgery among patients with hip and knee osteoarthritis,” Bone and Joint, vol. 104-B, no. 7, pp. 792–800, July 2022, doi: 10.1302/0301-620x.104b7.bjj-2021-1766.r1.
[9]P. Graham, “Progressive Osteoarthritis of the Hip.,” Orthopaedic Nursing, vol. 39, no. 4, pp. 270–272, July 2020, doi: 10.1097/NOR.0000000000000687.
[10]M. Reijman, “Determinants of progression of hip osteoarthritis,” Dec. 2004, [Online]. Available: https://pure.eur.nl/files/46296417/041201_Reijman.pdf
[11]L. Riglet et al., “Hip disability and Osteoarthritis Outcome Score trajectories and prognostic factors for functional decline: A 3-year follow-up study,” Annals of Physical and Rehabilitation Medicine, vol. 68, no. 1, pp. 101893–101893, Dec. 2024, doi: 10.1016/j.rehab.2024.101893.
[12]D. M et al., “Radiographic features predictive of radiographic progression of hip osteoarthritis.,” vol. 64, no. 12, pp. 795–803, Dec. 1997.
[13]A. Vahid et al., “Cohort profile: Worldwide Collaboration on OsteoArthritis prediCtion for the Hip (World COACH) - an international consortium of prospective cohort studies with individual participant data on hip osteoarthritis.,” May 2024, doi: 10.26181/25929535.
[14]E. A. Parker, A. M. Meyer, M. Nasir, M. C. Willey, T. S. Brown, and R. W. Westermann, “Abnormal Femoral Anteversion Is Associated With the Development of Hip Osteoarthritis: A Systematic Review and Meta-Analysis,” Sept. 2021, doi: 10.1016/J.ASMR.2021.07.029.
[15]A. Palmer et al., “Delayed gadolinium-enhanced mri of cartilage (dgemric) predicts the pattern of hip osteoarthritis progression at five-year follow-up,” Feb. 2018.
[16]R. Hidaka et al., “Development and accuracy of an artificial intelligence model for predicting the progression of hip osteoarthritis using plain radiographs and clinical data: a retrospective study,” BMC Musculoskeletal Disorders, vol. 25, no. 1, Nov. 2024, doi: 10.1186/s12891-024-08034-4.
[17]N. V. Bardakos and R. N. Villar, “Predictors of progression of osteoarthritis in femoroacetabular impingement: A RADIOLOGICAL STUDY WITH A MINIMUM OF TEN YEARS FOLLOW-UP,” Journal of Bone and Joint Surgery-british Volume, vol. 91, no. 2, pp. 162–169, Feb. 2009, doi: 10.1302/0301-620X.91B2.21137.
[18]Y.-J. Kim, “Hip Osteoarthritis: Bench to Bedside Perspective.,” Advances in Experimental Medicine and Biology, vol. 1402, pp. 125–133, Jan. 2023, doi: 10.1007/978-3-031-25588-5_9.
[19]T. Conrozier et al., “Quantitative measurement of joint space narrowing progression in hip osteoarthritis: a longitudinal retrospective study of patients treated by total hip arthroplasty.,” Rheumatology, vol. 37, no. 9, pp. 961–968, Sept. 1998, doi: 10.1093/RHEUMATOLOGY/37.9.961.
[20]N. E. Lane, M. C. Nevitt, M. C. Hochberg, Y. Y. Hung, and L. Palermo, “Progression of radiographic hip osteoarthritis over eight years in a community sample of elderly white women,” Arthritis & Rheumatism, vol. 50, no. 5, pp. 1477–1486, May 2004, doi: 10.1002/ART.20213.
[21]J. C. Baker-LePain and N. E. Lane, “Relationship between joint shape and the development of osteoarthritis,” Current Opinion in Rheumatology, vol. 22, no. 5, pp. 538–543, Sept. 2010, doi: 10.1097/BOR.0B013E32833D20AE.
[22]J. Shapira et al., “Radiographic factors associated with hip osteoarthritis: a systematic review.,” Journal of Hip Preservation Surgery, vol. 7, no. 1, pp. 4–13, Jan. 2020, doi: 10.1093/JHPS/HNZ073.
[23]T. Turmezei et al., “Quantitative 3D imaging parameters improve prediction of hip osteoarthritis outcome.,” Scientific Reports, vol. 10, no. 1, p. 4127, Mar. 2020, doi: 10.1038/S41598-020-59977-2.
[24]M. Reijman, J. M. W. Hazes, H. A. P. Pols, R. M. D. Bernsen, B. W. Koes, and S. M. A. Bierma-Zeinstra, “Role of radiography in predicting progression of osteoarthritis of the hip: prospective cohort study,” BMJ, vol. 330, no. 7501, pp. 1183–1185, May 2005, doi: 10.1136/BMJ.38442.457488.8F.
[25]J. Ledingham, S. Dawson, B. Preston, G. Milligan, and M. Doherty, “Radiographic progression of hospital referred osteoarthritis of the hip.,” Annals of the Rheumatic Diseases, vol. 52, no. 4, pp. 263–267, Apr. 1993, doi: 10.1136/ARD.52.4.263.
[26]J. J. Nepple, K. Thomason, T. W. An, M. Harris-Hayes, and J. C. Clohisy, “What is the utility of biomarkers for assessing the pathophysiology of hip osteoarthritis? A systematic review.,” Clinical Orthopaedics and Related Research, vol. 473, no. 5, pp. 1683–1701, Jan. 2015, doi: 10.1007/S11999-015-4148-6.
[27]P. Garnero, N. Charni, F. Juillet, T. Conrozier, and E. Vignon, “Increased urinary type II collagen helical and C telopeptide levels are independently associated with a rapidly destructive hip osteoarthritis,” Annals of the Rheumatic Diseases, vol. 65, no. 12, pp. 1639–1644, Dec. 2006, doi: 10.1136/ARD.2006.052621.
[28]C. X, “Is a biological marker for osteoarthritis within reach,” vol. 64, no. 10, pp. 562–577, Oct. 1997.
[29]Hosnijeh, Runhaar, van Meurs, and Bierma-Zeinstra, “Biomarkers for osteoarthritis: Can they be used for risk assessment? A systematic review.,” Maturitas, 2015, doi: 10.1016/j.maturitas.2015.04.004.
[30]B. Mazières et al., “Molecular markers of cartilage breakdown and synovitis at baseline as predictors of structural progression of hip osteoarthritis. The ECHODIAH Cohort,” Annals of the Rheumatic Diseases, vol. 65, no. 3, pp. 354–359, Mar. 2006, doi: 10.1136/ARD.2005.037275.
[31]D. M. J. Dorleijn, “Hip Osteoarthritis : symptomatic presentation and non-operative treatment,” Jan. 2017.
[32]N. K. Arden et al., “Can We Identify Patients with High Risk of Osteoarthritis Progression Who Will Respond to Treatment? A Focus on Biomarkers and Frailty.,” Drugs & Aging, vol. 32, no. 7, pp. 525–535, June 2015, doi: 10.1007/S40266-015-0276-7.
[33]T. Yasuda, “Early diagnosis and targeted intervention based on the pathogenesis of rapidly progressive osteoarthritis of the hip,” World journal of orthopedics, vol. 16, no. 10, pp. 108992–108992, Oct. 2025, doi: 10.5312/wjo.v16.i10.108992.
[34]H. Steingrebe, S. Spancken, S. Sell, and T. Stein, “Effects of hip osteoarthritis on lower body joint kinematics during locomotion tasks: a systematic review and meta-analysis,” Frontiers in sports and active living, Nov. 2023, doi: 10.3389/fspor.2023.1197883.
[35]A. Baily, R. S. S. S. Arachchige, M. Constantinou, and R. T. H. Cheung, “Differences in Temporal Spatial Gait Characteristics Between People With and Without Hip Osteoarthritis: A Systematic Review With Meta-analysis,” July 2023, doi: 10.2519/josptopen.2023.0017.
[36]H. Tateuchi, “Gait- and postural-alignment-related prognostic factors for hip and knee osteoarthritis: Toward the prevention of osteoarthritis progression.,” vol. 22, no. 1, pp. 31–37, June 2019, doi: 10.1298/PTR.R0003.
[37]H. Tateuchi, H. Akiyama, K. Goto, K. So, Y. Kuroda, and N. Ichihashi, “Clinical phenotypes based on clinical prognostic factors in patients with secondary hip osteoarthritis: preliminary findings from a prospective cohort study.,” Clinical Rheumatology, vol. 39, no. 7, pp. 2207–2217, Feb. 2020, doi: 10.1007/S10067-020-04988-7.
[38]A. Ocokoljic et al., “Short-term prediction of clinical and radiographic contralateral hip osteoarthritis after index total hip arthroplasty,” Archives of Orthopaedic and Trauma Surgery, vol. 145, no. 1, Dec. 2024, doi: 10.1007/s00402-024-05615-9.
[39]S. N. Hofstede, M. G. J. Gademan, T. P. M. V. Vlieland, R. G. H. H. Nelissen, and P. J. M. de Mheen, “Preoperative predictors for outcomes after total hip replacement in patients with osteoarthritis: a systematic review,” BMC Musculoskeletal Disorders, vol. 17, no. 1, pp. 212–212, May 2016, doi: 10.1186/S12891-016-1070-3.
[40]M. Wieczorek, C. Rotonda, F. Guillemin, and A.-C. Rat, “What Have We Learned From Trajectory Analysis of Clinical Outcomes in Knee and Hip Osteoarthritis Before Surgery,” Arthritis Care and Research, vol. 72, no. 12, pp. 1693–1702, Nov. 2020, doi: 10.1002/ACR.24069.
[41]A. Nilsdotter, I. F. Petersson, E. M. Roos, and L. S. Lohmander, “Predictors of patient relevant outcome after total hip replacement for osteoarthritis: a prospective study,” Annals of the Rheumatic Diseases, vol. 62, no. 10, pp. 923–930, Oct. 2003, doi: 10.1136/ARD.62.10.923.
[42]P. P. Cheung, L. Gossec, and M. Dougados, “What are the best markers for disease progression in osteoarthritis (OA),” Best Practice & Research: Clinical Rheumatology, vol. 24, no. 1, pp. 81–92, Feb. 2010, doi: 10.1016/J.BERH.2009.08.009.
[43]M. de Rooij et al., “Course and predictors of pain and physical functioning in patients with hip osteoarthritis: Systematic Review and Meta-Analysis,” Journal of Rehabilitation Medicine, vol. 48, no. 3, pp. 245–252, Mar. 2016, doi: 10.2340/16501977-2057.
[44]Iordache et al., “Unveiling Prognostic and Diagnostic Biomarkers in Knee and Hip Osteoarthritis: A Targeted Review.,” Discovery medicine, 2025, doi: 10.24976/Discov.Med.202537197.86.
ごあいさつ

長引いた痛みを一人で治すのは困難なことが多いです。
困ったときは自身で判断せずに適切な処置を受けるために専門家に相談しましょう。
もし、お近くにお住まいで、困っているならば、一度ひまわり接骨院までお問い合わせください。腰痛・坐骨神経痛の専門家の新幡が、ご相談に乗ります。
気軽にご相談ください。

新着情報・お知らせ
お気軽にお問合せください

お電話でのお問合せ・相談予約
<受付時間>
月~土
9:00〜13:00 /15:00〜19:00
※日曜・祝日は除く
フォームは24時間受付中です。お気軽にご連絡ください。
ひまわり接骨院

住所
〒213-0002
神奈川県川崎市高津区二子1丁目7−17 リバーサイドマンション杉崎 102
アクセス
二子新地駅 徒歩3分
駐車場:近隣にコインパーキングあり。自転車・バイクは店舗前に駐輪場がございます。
受付時間
月~土
9:00〜13:00 /15:00〜19:00
定休日
日曜・祝日

